Protein demand is hotter than ever, but not all proteins are created equal. Why more strategic protein innovators will be the ultimate winners in the GLP-1 nutrition space.
The Protein Gold Rush
The protein gold rush has CPG brands adding whey to everything from candy bars to pasta sauce. Convincing healthy people they need 40 grams of protein in their morning coffee can hardly be considered innovation – it’s just clever marketing. Companies are creating solutions for problems that don’t exist while ignoring a real, substantially more promising and profitable opportunity.
This explosion of high-protein everything is driven by influencer marketing and social media trends. Brand companies – essentially marketing entities that own no factories or equipment – ride these trends by contracting out production. When the trend fades, they’ll simply launch new brands to chase the next fad.
Meanwhile, ingredient suppliers invested heavily in protein production capacity to meet this hype-driven demand are now in desperate search of new applications. Most recently, the plant-based boom left these companies with specialized facilities, advanced protein processing capabilities, and long-term supply contracts, but plateauing demand.
The companies that are actually responsible for making real things in the real world – i.e., ingredient suppliers and co-manufacturers – have learned to serve whatever trend brand companies are chasing this quarter. They invest just enough capacity for today’s fad, knowing tomorrow will bring something different. This dynamic constrains genuine innovation. Why develop precise purification systems that maintain functionality when your customers’ marketing departments only care about riding the current hype train?
Current and former GLP-1 users are real people whose quality of life is directly tied to the food they consume. They need nutritionally dense food, not products plastered with meaningless claims. For companies tired of chasing fads, this represents something rare: medical need driving sustained demand. This is the market that justifies real innovation – where functionality and clinical outcomes matter more than marketing claims, where customers will pay premiums for products that actually work.
GLP-1s: A Tale of Two Markets
The rise of GLP-1 medications has created two distinct populations with urgent nutritional needs that standard protein products ignore.
Current Users: The Immediate Challenge
Muscle loss: Up to one-third of weight loss comes from lean tissue, not fat 1
Severe portion limits: Can only manage 4-6 oz of food per meal
GI sensitivity: Cannot tolerate traditional high-fiber foods or standard protein sources
Nutrient density imperative: With drastically reduced intake, every bite must deliver maximum nutrition
Former Users: The Growing Opportunity
85% discontinue within two years due to cost and insurance barriers 2
The protein-fortified food industry has mastered marketing but ignores quality. Most products deliver poor-quality protein that the body can barely use.
Here’s what matters: PDCAAS (Protein Digestibility Corrected Amino Acid Score) measures true protein quality. A score of 1.0 means optimal quality. Most trendy protein products don’t come close because high-quality protein is expensive, and the average consumer buying a protein cookie isn’t checking amino acid profiles.
This works when your customers are healthy people who don’t need extra protein. Most Americans already consume excessive protein. But GLP-1 users face genuine muscle loss risks and need products designed for medical nutrition, not Instagram appeal.
Key failures of current products:
Poor protein quality: PDCAAS scores of 0.1-0.2 when optimal is 1.0
Wrong format: 12-oz shakes when users can only manage 4-6 oz
Iron: 14 % of U.S. adults have absolute iron deficiency 7
Magnesium: ~45 % of Americans consume below the estimated average requirement 8
Ignores GI sensitivity: Denatured proteins slow digestion and reduce bioavailability; when fiber is present, it’s typically bulk-forming types that worsen symptoms by binding water, creating gas, thus slowing down already-slowed digestive systems
If an ingredient supplier develops proteins with optimized amino acid profiles and enhanced digestibility, they certainly won’t be advertising PDCAAS scores on TikTok. The non-medical market rewards trendy labels over technical specifications.
The High-Protein Market Opportunity
By The Numbers
By early 2024, roughly one in eight American adults had used a GLP-1 medication 9 – unprecedented adoption for a prescription obesity treatment. With 30 million Americans having tried GLP-1s 10 and an 85% discontinuation rate, we face a projected population of 25 million post-GLP-1 users within the next few years.
These aren’t casual dieters. They’ve experienced pharmaceutical-grade results and understand the stakes. Most importantly, their experience paying $1,200-1,500 monthly for medication creates powerful price anchoring. A specialized functional food program costing $150-200 monthly ought to be affordable by comparison.
Intersecting Opportunities
Regulatory catalyst: The FDA’s recent declaration ending GLP-1 shortages 11 access to affordable compounded versions. Millions must now choose between paying full price or discontinuing treatment.
Supply meets demand: Ingredient suppliers with excess capacity from the plant-based boom 12,13 possess the technical capabilities to create clinical-grade ingredients – they just need a market that values quality over marketing.
No dominant player:
Sports nutrition brands focus on athletes seeking muscle gains (supplements for enhancement, not medical needs)
Weight loss companies push meal replacements and appetite suppressants (often high fiber formulas that worsen GI distress)
Medical nutrition serves hospital patients with specific clinical protocols (requires prescription, too narrow for broad GLP-1 population)
None of these directly address the unique needs of current or former GLP-1 users – yet all the necessary components exist across these markets. This gap creates an opportunity for companies willing to combine clinical-grade quality with consumer-friendly formats.
Why Most Companies Will Miss This
Brand companies chasing protein trends are structurally unsuited for medical nutrition:
R&D priorities: Focus on taste and broad market appeal, not therapeutic efficacy
Distribution models: Built for high-velocity mass market, not premium, specialized products
Marketing metrics: Reward shelf turns and market share, not health outcomes
The short-term trap: Chasing quick profits through trendy products guarantees commodity pricing and thin margins. High-margin opportunities require long-term investment in clinical validation and precise manufacturing – commitments that quarterly-focused companies won’t make
The companies that recognize this gap – and have the technical capability to bridge it – will define the next decade of functional food.
The Path to Prosperity
Success in this market requires rethinking fundamental assumptions about product design:
Format is everything: Products must work within 4-6 oz portion limits while delivering the 25-30g of quality protein needed per meal to stimulate muscle protein synthesis 14. Plus, they need to include essential micronutrients.
Quality over marketing: Pre-digested proteins, gentle fibers, bioavailable micronutrients – the ingredients that matter won’t fit on a trendy label.
Distribution strategy: Direct-to-consumer or specialty channels that allow for education and premium pricing.
Companies positioned to win aren’t necessarily those with medical food experience – they’re those willing to treat this as the medical nutrition challenge it is. A nimble contract manufacturer could partner with the right brand. An innovative ingredient supplier could develop turnkey solutions.
Seize the Moment
The market is developing rapidly. Regulatory changes and discontinuation patterns are creating new cohorts of former users each month.
The convergence of opportunities makes the current moment a unique – and fleeting – one:
25 million consumers with proven premium spending capacity
Ingredient suppliers with excess capacity and technical capabilities
No established market leader
Innovation comes from combining three successful models (D2C distribution, medical nutrition, premium pricing) to create a new product category
For ingredient suppliers and contract manufacturers tired of chasing quarterly fads, this represents something rare: a chance to build lasting value by solving real problems.
The question isn’t whether this market will develop – it’s who will capture it first.
Interested in exploring how your capabilities could serve this emerging market?
Contact David Goulder to discuss the technical and market requirements necessary to seize this moment.
Lance Lively is the Founder of The Gut Punch, a platform investigating the intersection of food and health. He’s served as a senior leader at a number of venture-backed biotechnology companies. A Princeton and Wharton graduate, he focuses on human health, novel modalities to improve wellness, and the science of addiction.
David Goulder is the founder of Food Science and Applied Research Consulting, with 11 years of experience in food science and technology. He works at the intersection of science, strategy, and product development – helping teams solve complex technical challenges efficiently, from ingredient functionality and formulation to integrating new research and scaling innovation. David holds a BS and MS in Food Science and Technology.
My interview with Marc Washington, Founder & Executive Chairman of SuperGut.
SuperGut: Marc Washington
What separates a truly transformative health brand from the endless sea of wellness products promising to cure all maladies?
Why do some founders build category-defining companies, while others with nearly identical ingredients fade into obscurity?
And what happens when years of scientific groundwork suddenly collide with a metabolic revolution that completely reshapes people’s relationships with food?
In case you haven’t noticed, fiber and GLP-1s are both having major cultural moments. And SuperGut, whether through prescience or providence, spent years developing gut-healthy fiber blends and conducting gold-standard clinical trials – long before Ozempic became a household name.
I recently joined Alex Shandrovsky, host of the Investment Climate Podcast, for a conversation with Marc Washington, founder and executive chairman of SuperGut.
Our discussion digs into the balancing act between scientific rigor and market momentum, the hard decisions around investing in clinical validation versus splashy marketing, and what it takes to carve out real differentiation in a world where a new “natural GLP-1” copycat emerges every week.
And as Marc transitions from CEO to Executive Chairman, we tackle the ultimate question that haunts every founder as they hand over the reins: how will you know whether you’ve built an enduring brand that will stand the test of time?
Inside America’s broken drug pricing system, and why health insurers are the men behind the curtain
There’s More to Drug Pricing than Meets the Eye
In last month’s investigation, we exposed the devastating impact of the FDA’s decision to end access to compounded GLP-1 alternatives, forcing millions of Americans to confront the shocking reality of $1,000+ monthly price tags for brand-name weight loss and diabetes medications.
We explained how manufacturers set astronomical list prices, how other countries pay a fraction of what Americans pay, and how insurers rarely cover these drugs for obesity despite their proven effectiveness.
But there’s another critical piece to this affordability puzzle: the hidden middlemen.
The Hidden Layer
While pharmaceutical manufacturers like Novo Nordisk and Eli Lilly certainly bear responsibility for setting high list prices for drugs like Ozempic, Wegovy, Mounjaro, and Zepbound, a complex and opaque network of intermediaries – particularly Pharmacy Benefit Managers (PBMs) – wields extraordinary influence over what patients ultimately pay and whether they can access these medications at all.
Drugmakers argue that U.S. prices are high because of the unique American system of rebates and middlemen. In a 2024 Senate hearing, Novo Nordisk’s CEO testified that “we pay 75 cents of every dollar of medicine we sell back into this complex system in rebates, discounts, and fees.” 1 In other words, only 25% of the gross revenue from Ozempic/Wegovy might actually be kept by Novo Nordisk; the rest is absorbed by intermediaries in the supply chain.
That “complex system” includes PBMs negotiating rebates, insurers and Third-Party Administrators (TPAs) administering plans, and brokers steering employer insurance plan decisions. Each intermediary takes a slice.
When competition is limited (as with brand-name GLP-1s under patent) and cheaper workarounds like compounding are eliminated, the leverage of these middle players grows. With no low-cost alternative available, all transactions must flow through the standard distribution and insurance channels – where middlemen can impose their mark-ups, fees, or negotiated spreads.
The result is a U.S. market where list prices soar, even if net prices after rebates are somewhat lower – and patients without strong insurance coverage can be left with unaffordable bills.
Pharmacy benefit managers (PBMs) are often singled out in discussions of high drug costs – and for good reason. PBMs manage prescription drug benefits for insurers and employers, deciding which drugs are covered (formularies) and negotiating rebates and discounts with drug manufacturers.
Health plans (i.e. employers and insurers) often choose PBM services based on criteria like rebate guarantees, formulary breadth, and administrative cost, which pressures PBMs to maximize rebates. PBMs also compete to secure exclusive arrangements with large buyers by offering bigger savings, which often means bigger rebates.
In theory, PBMs are meant to leverage volume to lower net costs for health plans. In practice, their business model can create perverse incentives that inflate list prices.
Rebate Structures and Formulary Control
PBMs typically negotiate hefty rebates from manufacturers of expensive brand-name drugs in exchange for favorable placement on the formulary, a list of medications that a specific health insurance plan or PBM covers.
These rebates are paid by the manufacturer to the PBM after the sale and are often a percentage of the drug’s list price. This means a PBM’s revenue from a drug can increase if the manufacturer raises the list price, since a higher price yields a larger rebate (even though the net price to the insurer and insured patients may remain unchanged).
According to an FTC investigation, the “Big Three” PBMs (CVS Caremark, Express Scripts, and OptumRx) – which together manage about 80% of U.S. prescriptions 2 – have created a “perverse drug rebate system” that prioritizes high rebates over low list prices 3.
Case Study: Insulin
The FTC’s 2024 complaint against PBMs alleges they “rigged” the system so that drugs with higher list prices (and thus higher rebates) are favored, while lower-list-price alternatives are excluded, ultimately artificially inflating drug costs 4.
In the case of insulin, even when lower-priced versions came to market, PBMs kept them off formularies in favor of higher-priced, rebated products. This strategy allowed PBMs and their affiliated rebate intermediaries to “line their pockets while patients are forced to pay higher out-of-pocket costs,” according to the FTC 5.
Pricing Power and Rebate Walls
Because PBMs control formulary access for millions of patients, manufacturers feel compelled to offer large rebates to secure or maintain favorable placement. A high-demand drug like a GLP-1 agonist effectively faces a “pay-to-play” system.
If Novo Nordisk or Eli Lilly didn’t offer substantial rebates, a PBM could exclude their drug or put it on a higher copay tier in favor of a competitor that offers a bigger rebate. This has led to what some call “rebate walls,” 6 where dominant products (with high list prices and rebates) block cheaper would-be rivals from getting traction.
The result is inflated list prices across the board. So long as PBMs are evaluated by plan sponsors on how much rebate dollars they secure, they have a motivation to prefer high-price/high-rebate drugs to lower-cost drugs that don’t throw off as much rebate, even if the lower-cost drug might save the health plan money overall.
So… Who Owns the PBMs?
The largest PBMs have merged with insurance companies and pharmacy chains (surprise!), creating massive healthcare conglomerates:
CVS Caremark is part of CVS Health, which owns Aetna insurance and CVS pharmacies
Express Scripts is owned by Cigna
OptumRx is part of UnitedHealth Group
This integration creates additional profit opportunities. PBMs steer patients to higher-revenue drugs while blocking competitor pharmacies from offering discounts 7.
Application to GLP-1 Drugs
For GLP-1 medications, manufacturers have openly asserted that a similar perverse dynamic is at play. Lars Fruergaard Jørgensen, CEO of Novo Nordisk, testified during a U.S. Senate hearing that the high U.S. list price for Ozempic/Wegovy was driven by PBM negotiations, not production costs 8.
Jørgensen noted that simply lowering the list price would likely backfire because PBMs “often limit access to drugs with lower list prices because they receive less financial benefit from them.” 9 This rebate-driven distortion is a key reason U.S. prices are far above those in Europe, where such rebate middlemen play a smaller role.
The PBM industry argues that manufacturers alone set the prices and that PBMs actually return most savings to patients or payers. In the recent Senate hearing, major PBMs stated they would welcome lower list prices for GLP-1 drugs, and a list price cut wouldn’t harm formulary placement so long as the net cost for their insurance clients remains unchanged 10.
In reality, PBMs wield enormous pricing power over GLP-1 drugs by controlling access and playing manufacturers off one another. While PBMs are motivated to secure the lowest net cost for their clients, the opaque rebate system makes it hard to tell if a truly lowest net cost is achieved and allows PBMs to take a fat cut along the way.
As long as PBM revenue comes from a slice of the drug price, their actions will tend to favor higher prices.
Third-Party Administrators (TPAs): Hidden Costs in Plan Administration
When an employer self-funds its health benefits – paying claims with its own dollars rather than buying insurance – it typically hires a third-party administrator (TPA) to run the health plan. TPAs handle claims processing, provider networks, utilization management, and often the pharmacy benefit – either directly or via a PBM partner.
The expectation is that a TPA will act in the employer’s and members’ best interest to manage costs. However, many TPAs are actually divisions of major insurance companies (surprise!). For example, Anthem’s affiliate administers many employer plans, even if the plan is self-funded 11.
TPAs therefore have their own insurance-aligned incentives and conflicts of interest that can drive up spending, unbeknownst to employers.
Influence on Coverage and Utilization
TPAs help employers design their benefit plans – including whether or not to cover certain medications like weight-loss drugs, and under what conditions. Their advice might be colored by cost considerations (GLP-1 coverage can significantly increase claims cost) but also by competitive pressures (employers want to attract talent with good benefits).
TPAs might impose prior authorization or clinical criteria to control utilization. Importantly, if a TPA is aligned with a PBM, it may follow the PBM’s formulary and coverage rules, which, as discussed, might favor certain high-cost drugs. For instance, if a compounded semaglutide was available and cheaper, a TPA might still exclude it as “not FDA-approved” (and indeed many did, even before FDA’s crackdown, albeit for liability concerns).
Opaque Fees and Secret Overpayments
A less visible issue is how some TPAs extract value through the pricing of claims and services. Because TPAs directly negotiate with providers and PBMs with limited oversight from employers, they might have opportunities to financially benefit from this information asymmetry.
For example, there have been cases where an insurer acting as a TPA negotiated discounts with hospitals or pharmacies but did not fully pass those savings to the employer’s plan. In one lawsuit, a union health fund accused Anthem (now Elevance Health) of unlawfully applying only part of a hospital discount and retaining the difference, effectively overcharging the self-funded plan 12.
Such hidden overpayments can go undetected when TPAs refuse to share detailed claims data. Historically, “gag clauses” in contracts prevented employers from seeing price details. Congress banned these gag clauses in 2021, but compliance remains spotty 13.
The Georgetown University Health Policy Institute has noted multiple court cases in recent years that uncovered questionable TPA conduct, such as hiding data or failing to act in the plan’s interest 14. These practices contribute to excessive health care spending for employers: if a TPA can get away with a slightly higher payment here or there, the employer may never know – but everyone’s premiums and costs inch upward.
TPAs might not grab headlines like PBMs do, but they play a significant role in plan costs. Their influence is more about how costs are managed or hidden rather than drug pricing per se. When it comes to expensive drugs like GLP-1s, there’s even more room for middlemen like TPAs to inflate fees and increase their take – at our collective expense.
Insurance Brokers and Consultants: Incentivizing High-Cost Plans
Employers sponsoring health insurance, whether fully-insured or self-funded, often rely on benefits brokers or consultants to advise them. These brokers help design benefit packages and recommend insurers or administrators. They are supposed to find the best value for the employer and employees.
However, the traditional compensation structure for brokers can pose a serious conflict of interest: most brokers are paid commissions and bonuses by the health insurance industry (surprise!). As a result, brokers may have a financial incentive to favor plans that are more lucrative for them – which predictably correlates more expensive plans that increase overall insurance coverage costs.
How Brokers Get Paid
Typically, when an employer buys a health insurance policy (for smaller companies) or contracts for services (for larger plans), the broker receives a commission from the insurer or vendor. This commission is often calculated as a percentage (e.g. 3–6%) of the total premium or contract value 15. The higher the premium or cost, the higher the broker’s commission.
On top of base commissions, insurers and PBMs commonly offer brokers additional incentives: for example, bonuses for bringing in large groups or keeping clients with the same insurer and even lavish perks like paid trips or exclusive events for top-performing brokers.
A 2019 investigative report by ProPublica revealed brokers were being wooed with “six-figure bonuses to swanky island getaways,” a practice critics called a “classic conflict-of-interest” that can put industry profits above clients 16. Until recently, much of this went undisclosed to employers.
Brokers’ built-in biases towards more expensive plans aren’t limited to insurance plans – this bias can extend to pharmacy benefits as well. As ProPublica reported, “each service provider may provide payments to brokers unknown to the employer” 17 – including PBMs paying a fee for every prescription filled or TPAs paying brokers for each employee added to their plan.
Impact on GLP-1 Coverage Decisions
When it comes to high-cost drugs like GLP-1 agonists, brokers influence the overall plan design and the choice of insurer/PBM. If an employer is debating whether to cover weight-loss medications, a broker’s guidance matters.
Ideally, the broker would present the cost impact and pros/cons objectively. But if, say, the broker’s compensation from the health plan will increase as claims (and premiums) increase, the broker might be less motivated to help the employer contain those costs.
However, brokers know that an unhappy workforce or an uncompetitive benefits package could cost them the client. GLP-1 drugs give brokers a chance to kill two birds with one stone.
Brokers might actually encourage adding a popular benefit like coverage for Wegovy for obesity because it makes the overall plan more attractive. And if the employer’s costs – and thus the broker’s commission – just so happen to increase as a consequence? All the merrier.
Changes and Transparency
Recognizing these conflicts, policymakers have taken steps to shine a light on broker compensation. A new federal law (enacted as part of the Consolidated Appropriations Act, 2021) now requires brokers and consultants to disclose to employers any direct or indirect compensation they receive from insurance carriers, PBMs, or other vendors 18.
Still, the legacy of the commission system means many brokers are essentially encouraged to keep healthcare spending and premiums high. Brokers are not necessarily behind the sky-high price of GLP-1 drugs. But they are unlikely to strongly advocate for aggressive cost-reducing measures if such efforts reduce their own earnings.
The Economics Behind Inflated Prices
Stepping back, we see two major patterns that explain why the U.S. struggles with high drug prices versus other industrialized nations:
Many healthcare intermediaries are compensated in ways that scale with the price of the product or service.
Many healthcare intermediaries are either directly controlled or financially incentivized by healthcare insurance companies.
This latter observation is really worth unpacking. Not only are these healthcare middlemen heavily consolidated within their service area (for instance, the three biggest PBMs control nearly 80% of the market 19), but these middlemen are also vertically integrated with insurers and pharmacies – resulting in healthcare oligopolies.
To demonstrate the immense power that vertical integration affords, let’s study the world’s second largest healthcare company, CVS Health:
CVS Health owns CVS Caremark (a PBM), CVS Pharmacy (retail and specialty pharmacies), Aetna (a health insurer), Wellpartner (a TPA for 340B services) 20, and Oak Street Health (a Medicare-focused primary care provider)
CVS Caremark steers prescriptions directly into its own CVS Pharmacy networks, effectively sidelining independent pharmacies and other competitors.
CVS Caremark can mandate or incentivize Aetna’s vast insurance customer base to use CVS Pharmacies, limiting competition and allowing them to keep profits in-house.
CVS Health has been accused of forcing 340B entities to use its TPA Wellpartner, “effectively forcing covered entities to either forgo substantial savings from the 340B program… or forgo utilization of another TPA that might offer better pricing, quality, or service.” 21
CVS-owned Oak Street Health has been accused of providing health insurance brokers illegal kickbacks in exchange for steering Medicare Advantage enrollees towards Oak Street 22.
This interconnected ecosystem – insurers, PBMs, pharmacies, TPAs, and brokers – creates a powerful cycle of cost inflation, limiting true market competition and keeping American drug prices significantly higher compared to those in other industrialized nations.
Therefore, the nation’s GLP-1 affordability crisis is as much about perversely incentivized middlemen as it is about any one pharmaceutical manufacturer. Unless or until lawmakers, employers, and other stakeholders demand deeper transparency and realignment of incentives, these new weight-loss and diabetes treatments will remain out of reach for too many Americans.
It’s easy to see why each middleman behaves as it does – everyone is just following the money. But after mapping out the pipeline, from manufacturer to insurer to PBM to TPA to broker, it’s painfully clear that the voices that matter the most – those of patients and plan sponsors – aren’t getting much say in how that money flows.
Perhaps the real question, then, is how much longer can this elaborate chain of insurance-controlled profiteers hold out against an increasingly desperate public that is losing GLP-1 coverage and on the financial brink?
Insights from food & health industry leaders at the MISTA Healthy Nutrition Symposium
The GLP-1 Disruption Through the Eyes of Experts
The food industry is facing an unprecedented challenge: a new class of drugs is dramatically changing how people eat. GLP-1 agonist medications – like Ozempic, Wegovy, and Mounjaro – have emerged as powerful appetite suppressants by mimicking a gut hormone that regulates hunger. Originally developed to treat diabetes, they are now reshaping what consumers buy, how they snack, and how companies innovate.
It’s one thing for a new diet craze to ask consumers to choose differently; it’s another for a prescription drug to make them feel differently. As appetite literally shuts down and satiety spikes, major food and beverage categories feel the impact.
Analysts warn billions of dollars of consumer spending are up for grabs. KPMG projects consumers may spend $48 billion less on food and drink each year for the next decade due to GLP-1 use 1. Some of the world’s biggest players – Nestlé, Coca-Cola, Danone, Conagra – are already pivoting to meet the GLP-1 moment.
“We don’t want to be the last guy,” admits Conagra Senior VP Bob Nolan.
So how should the food industry respond? To explore this question, I convened a panel of four experts at MISTA’s 2025 Healthy Nutrition Symposium:
Cate Ward (Semper Organics): Scientist, dietitian, and Stanford University researcher whose work intersects nutrition and microbiome science.
Jenny Zegler (Mintel): Director of global food and drink research at Mintel with 17 years covering food and beverage innovation.
Emilie Fromentin (Givaudan): Head of Explore Health, Functional, and Color at Givaudan, a global leader in flavors, ingredients, and nutritional solutions.
Rocio Martin (Danone): Senior Director of Life Science Innovation at Danone, focused on biotics, proteins, and overall health benefits in food.
Our conversation reveals how GLP-1 medications are reshaping consumer behaviors at a biological level – and how food companies can position themselves to not only survive but thrive in this new world.
The Physiological and Behavioral Impact of GLP-1s on Food Consumption
Changing the Fundamentals of Consumption
The physiological punch of GLP-1 agonists is impossible to ignore. By slowing gastric emptying and blunting hunger signals, these drugs lead people to feel full on far less food.
“These medications reduce the craveability of food and increase satiety,” says Cate Ward. “But they also come with side effects like GI symptoms and nausea.”
Data from Mintel underscores how this plays out in daily eating habits. According to Jenny Zegler:
“Smaller portions are the new norm for GLP-1 users. Yet our research finds 51% of U.S. adults on these drugs increased their snacking compared to the previous year, far surpassing the 25% figure for all U.S. adults.”
This contradiction – snacking more, yet eating smaller total quantities – suggests consumers are reorganizing how and when they eat, rather than blindly restricting all food. Danone’s internal data points to another shift:
“GLP-1 users are consuming smaller meals but more frequently, and more healthy snacks – fruits, vegetables, dairy, high-protein, and fiber-rich foods – while decreasing processed items, sweets, and alcohol,” explains Rocio Martin.
In fact, many GLP-1 households are increasing their spend on yogurt, ready-to-drink protein shakes, and nutrition bars at higher rates than non-users. A recent Cornell study bears this out: in the first six months, savory snack buys dropped 11% and sweet baked goods 9%, while spending on healthy staples climbed 2.
Changes in Grocery Spending Six Months Post GLP-1 Adoption by Category. The No-Hunger Games: How GLP-1 Medication Adoption is Changing Consumer Food Demand
Evolution of Eating Patterns Across the GLP-1 Journey
Food preferences also shift throughout a GLP-1 user’s journey. Early adopters often battle nausea and intense fullness, then pivot to optimizing diet quality once maintenance sets in.
“They start caring about not losing too much muscle and ensuring adequate nutrients in a limited diet,” says Ward, who sees many GLP-1 patients in her private practice. “After stopping the medication, some are determined to keep the weight off by improving diet quality.”
Zegler notes Mintel found that 12%+ of weight-managing adults have previously used GLP-1 drugs, roughly the same share as those currently on them 3. That suggests plenty of former patients need on-going nutritional support.
“There’s a real opening for foods and supplements that replicate that satiety benefit,” Zegler says, “particularly for people no longer on the drug but still keen to manage weight.”
KFF Health Tracking Poll May 2024: The Public’s Use and Views of GLP-1 Drugs
Changes in Taste Perceptions and Food Desires
A less-discussed twist is how these medications may dampen taste perception itself. Emilie Fromentin points to a recent study in Physiology & Behavior showing depressed perception of all five taste qualities – sweet, sour, salty, bitter, savory – among GLP-1 users 4.
“We need more research,” says Fromentin. “But anecdotally, patients report they just don’t crave sweets or certain rich flavors as strongly, which might explain why they gravitate to fresh produce and yogurt.”
Meanwhile, muscle loss remains a key concern. Clinical data shows 15% to 60% of total weight lost on GLP-1 drugs can be lean mass 5 – which has massive potential metabolic downsides.
“Beyond its structural roles, muscle influences glycemic control and metabolism,” says Martin. “Users should focus on high-quality protein intake and resistance training to minimize lean mass loss.”
Some scientists even recommend whey over casein-based proteins, given casein’s clotting effect in the stomach might amplify fullness and reduce intake of crucial nutrients.
Unexpected Changes in Consumer Behavior
Given these complexities, the consumer journey isn’t straightforward. Severe nausea can make patients seek bland, fortified foods on “new dose days,” while intermittent usage patterns mean people may “go on and off” the drug, as Fromentin points out.
“That’s another opportunity: post-treatment solutions. Cost is a big factor, so we expect waves of usage,” she adds. “Food companies should track new drug releases and remain agile.”
Commercial Implications and Market Adaptation
How Early Movers Are Responding
Faced with these seismic shifts, big players are experimenting with different strategies. Danone took the lead in proactively spotlighting existing products suited to GLP-1 users. A dedicated page on its website showcases protein-rich yogurts and shakes.
“Danone NA highlights items that address GLP-1 challenges – muscle preservation, bone density, minimal added sugar,” says Martin. “Coca-Cola touts that two-thirds of its portfolio has low or no calories, Campbell’s pushes nutrient-rich soups, and Nestlé just launched an entire new brand – Vital Pursuits – targeting this demographic.”
Vital Pursuits focuses on portion-controlled frozen meals (250–400 calories) high in protein and fiber. The brand doesn’t mention GLP-1 meds explicitly; it simply bills itself as “High Protein, Portion Aligned, Essential Nutrients.”
On the other end of the spectrum, Conagra is testing an “ON TRACK – GLP-1 Friendly” icon for select Healthy Choice meals, calling out high-protein, high-fiber recipes right on the package. Conagra wants to help GLP-1 users spot these products immediately. It’s a bold approach – more transparent than Nestlé’s stealth branding, but also riskier.
New Foods and Supplements for GLP-1 Users
The lines between food and supplement are blurring. Many GLP-1 users need added nutrients to compensate for lower intake.
“There are parallels between GLP-1 and bariatric surgery patients – both need daily multivitamins,” notes Zegler. “GNC has created dedicated sections for these customers, offering muscle-health, hydration, and energy formulations.”
Danone, for its part, is betting on functional dairy, high-protein snacks, and specialized lines to combat muscle loss. Martin believes in packaging these solutions with education:
“Should you create a specific GLP-1 product line or simply adapt existing SKUs? Either way, bridging knowledge gaps – on muscle preservation, GI side effects, or nutrient deficits – is key.”
Meanwhile, Semper Organics (where Ward works) is exploring how mushrooms and fermentation can deliver nutrients in compact volumes. Ward sees consumer interest in functional foods:
“With new dosage levels come intense side effects, and patients crave gentle, tummy-friendly solutions – fortified crackers, ginger-infused soups, or microbe-based snacks to help with GI symptoms.”
Consumer Response to New Products
So far, the data on consumer response is limited but telling. Some early adopters want explicit labeling (“GLP-1 Friendly!”), but others prefer stealth.
“80% of GLP-1 users are looking for products marketed for their needs, but only 21% want it outright stated on the label,” Martin says, citing a recent Danone-commissioned survey. “It’s a delicate balance: you have to guide them without making them self-conscious.”
Ward sees a clear split: “Some patients want super-clean, less-processed food; others still need convenience. They just want better macros, vitamins, and easy digestion.”
Product Development & Innovation Strategies
Addressing GLP-1 Users Without Alienating Others
Food giants are currently facing a major marketing question: How to reach GLP-1 consumers while ensuring their products also remain appealing for general consumers?
“Using calls like ‘portion aligned’ or ‘excellent source of protein’ resonates with GLP-1 users without explicitly calling them out,” explains Martin. “Retailers can also create store/website sections to cluster these products – think of Walmart’s online gating strategy. But direct labeling can backfire.”
Nestlé tries a middle path with Vital Pursuits, including a QR code that leads curious consumers to a page explaining how the meals are ideal for smaller appetites. By contrast, Conagra’s ON TRACK logo is an experiment in radical transparency.
Specific Product Opportunities for GLP-1 Patients
The panelists agree that muscle preservation is top priority. That means high-quality proteins, plus fiber and probiotics for GI health. Smaller portion sizes are also a must.
“We need to pack nutrients in every bite – whether it’s a compact meal, or a snack that’s bland enough to help with nausea but still delivers protein,” says Ward.
Healthy fats, minimal sugar, plus vitamins D, B12, and iron are also on the radar. Fromentin underscores the potential of advanced flavor systems to help ensure GLP-1 patients are receiving adequate nutrition:
“Taste solutions can help keep the eating experience pleasant despite GLP-1 patients’ reduced taste perception. We’re also leveraging technologies that have been historically utilized for specialized medical nutrition – such as compacting nutrients into small volumes.”
These recommendations align with research showing that 56% of GLP-1 users say they’re opting for more nutritious foods over junk food, 66% report cutting back on soft drinks and alcohol, and 38% are increasing their protein drink intake 6.
Lessons From Previous Health Trends
Our experts see parallels with earlier diet booms, but also big differences. Low-carb, low-fat waves primarily hinged on consumer willpower. GLP-1 reconfigures biology itself.
“We might see some reversion to old preferences, like low-fat to lessen nausea and GI distress,” says Ward, “but each patient’s needs differ drastically. One-size-fits-all solutions won’t cut it.”
Zegler emphasizes:
“Consumers – on GLP-1 or not – still have personal preferences about what to add or avoid. High protein, hydration, and fruits and veggies remain universal for weight loss. The difference is, GLP-1 users feel satisfied faster.”
Long-Term Solutions Beyond the GLP-1 Moment
Looking ahead, new classes of weight-loss drugs may address muscle loss or further alter appetite. Fromentin points out that global expansion is inevitable, with cost the biggest barrier abroad:
“Companies should plan for the day these meds become more affordable or covered by insurance in Europe, Latin America, or Asia.”
Ward adds:
“You can’t just design for the GLP-1 moment,” says Ward. “What about transitioning off the meds? Or layering with new treatments that preserve muscle? Or conversely, products to support lifetime users? Products that adapt with the consumer’s journey will have staying power.”
Zegler reminds us:
“GLP-1 is another tool in the weight-management toolbox. With research pointing to many users only using GLP-1s for a short period of time, it’s smartest for companies to build products that fit the foundations of health and wellness – protein, fiber, hydration, and natural ingredients – rather than try to add labels and formulations to align with the latest craze in weight loss.”
Martin echoes this sentiment:
“Don’t limit yourself to ‘for GLP-1 users only.’ Post-treatment might be even more critical, especially if people rebound or look for gentle ways to keep weight off.”
A Call to Action for the Food Industry
Collectively, the panel drives home a stark reality: GLP-1 drugs have handed consumers a powerful tool to control hunger, and now the ball’s in the food industry’s court to meet consumers’ needs for healthier, more nutritious options. The opportunity is huge, but seizing it requires swift and strategic moves:
Embrace Nutrient Density Every product – from snacks to meals – should deliver more protein, fiber, and micronutrients per bite. This benefits GLP-1 and non-GLP-1 customers alike.
Right-Size Portions and Packaging If shoppers only want a few bites, give them portion-aligned formats. Single-serve packaging or 100-calorie packs can prevent waste and encourage mindful eating.
Communicate Benefits, Not Medications Consumers want help finding muscle-supporting, GI-friendly, or portion-aware products, but don’t necessarily want “GLP-1” emblazoned on the label. Emphasize function (high protein, nutrient-dense) rather than referencing the drug.
Invest in R&D and Partnerships Collaborate with nutritionists, ingredient suppliers, and even fitness brands to tackle issues like muscle loss, taste modulation, and side-effect management. Leverage emerging “compacting” technologies from specialized medical nutrition fields.
Anticipate Future Drug Classes Already, combination therapies are in trials, some addressing muscle atrophy or boosting metabolism further. Stay agile, as the “appetite puzzle” could keep evolving.
Above all, the best hedge is to create robust, healthy foods that align with consumers’ broader wellness goals.
Companies that double down on ultra-processed, empty-calorie products and ignore the GLP-1 trend risk slowly declining as consumers reallocate their dollars. In contrast, those who innovate with quality and wellness in mind can capture not only the GLP-1 segment but also the broader shift of consumers who, with or without medications, want to eat more healthfully.
The food industry stands at a crossroads. GLP-1 drugs have handed consumers a powerful tool to control their eating – and they are using it. Rather than lamenting that people are buying fewer snacks or beverages, smart brands see a chance to become partners in consumers’ health journeys. By delivering products that align with new eating habits, companies can maintain relevance and loyalty.
To the food industry professionals, it’s time to meet the moment: adapt boldly, innovate relentlessly, and help shape a healthier, more resilient food culture for all. Your consumers’ appetites may be shrinking, but their expectations are not – and meeting those expectations is the path to thriving in this new world.
The FDA just ended access to cheaper GLP-1 alternatives – why are the brand-name drugs so expensive?
The End of GLP-1 Compounding Loophole
The Food and Drug Administration’s February 2025 declaration that Novo Nordisk’s Ozempic and Wegovy are no longer in shortage 1 has set off alarm bells for millions of Americans who relied on cheaper, compounded versions of these life-changing medications. This announcement – coming on the heels of a similar ruling in January for Eli Lilly’s tirzepatide (Mounjaro/Zepbound) 2 – effectively ends the regulatory leeway that allowed compounding pharmacies to produce lower-cost semaglutide or tirzepatide. Now, patients who had been paying a fraction of the official price must grapple with $1,000+ monthly costs or risk discontinuing therapy altogether.
Given this shock to the system, it’s worth reexamining a few simple and fundamental questions: why are brand-name GLP-1 drugs so expensive? Why are these astronomical prices a uniquely American phenomenon? And how can we break the cycle and ensure afforable, ready access for the patients who most need these medications?
Hims & Hers, a telehealth firm that previously sold compounded semaglutide, saw its stock plummet by 26% following the FDA announcement 3. The company had reported $1.5 billion in annual revenue in 2024 – a 69% increase from the prior year 4 – fueled largely by demand for affordable GLP-1 alternatives. Although Hims & Hers initially pledged to keep offering personalized options, it later confirmed it would discontinue compounded semaglutide by the end of Q1 2025 5.
Hims & Hers five-year net income chart(source: Sherwood).
Alliance for Pharmacy Compounding CEO Scott Brunner worries about the human toll of the ruling. “All we can do now is watch what happens as patients hear the news and try to get a new prescription for the FDA-approved drug.” He notes the “sticker shock” of branded semaglutide puts it out of reach for many patients 6.
Some compounders are challenging the decision in court. The Outsourcing Facilities Association and Texas-based FarmaKeio Superior Custom Compounding filed suit in Fort Worth, alleging that the FDA is “dismissing evidence that the shortage persists” and removing the drugs from its shortage list “without notice-and-comment rulemaking.” 7
Price Shock for Patients
“Today is not a good day for those suffering from chronic disease,” said Noom CEO Geoff Cook, whose digital health company prescribes compounded semaglutide 8. The FDA’s wind-down period allows compounders until April 22 to stop selling copycat versions 9 – giving patients and providers only a brief window to make alternative arrangements. For many, that means confronting the stark reality that the brand-name drugs come with punishing price tags.
While it addresses legitimate safety concerns surrounding unregulated “knockoff” medications, the FDA’s decision exposes deeper flaws in the American healthcare system. It forces a reckoning with short-term economic incentives that render revolutionary treatments inaccessible, even when the long-term medical and financial benefits could be enormous.
Jason Krynicki, Bariatric Insurance Coordinator at Robert Wood Johnson University Hospital and National Board Member of the Obesity Action Coalition, has experienced the economic anxiety of sudden GLP-1 price increases first-hand: “I lost my personal coverage in February 2023 at RWJ – they’re no longer covering obesity medications. I had to tap into my own savings to cover my GLP-1 drugs, which has put me in a really tough spot,” he explains.
Now, with cheaper compounding options phased out, millions of patients who have been taking compounded GLP-1s in the US are about to experience the same price shock. These patients must either pay significantly higher prices for brand-name products, fight for insurance coverage that often doesn’t exist, or give up treatment altogether.
The Price-Value Disconnect: Why GLP-1 Drugs Cost So Much
Manufacturer Margins: A Legal Monopoly
(Source: JAMA Netw Open. 2024;7(3):e243474).
Scrapping cheaper compounded versions shines a harsh spotlight on the massive disconnect between production costs and retail prices for GLP-1 medications. In 2023, a Yale study revealed that a monthly supply of semaglutide can be manufactured for as little as $0.89 to $4.73, yet the list price in the U.S. can exceed $1,000 10. This 21,000% markup is often justified by pharmaceutical firms as necessary to cover R&D costs, clinical trials, and the “innovation premium” that patents provide until the early 2030s.
Novo Nordisk and Eli Lilly have capitalized on this exclusivity to maintain premium pricing and post record profits. Novo reported more than $21 billion in combined 2023 revenue for semaglutide (Ozempic, Rybelsus, and Wegovy) alone 11. “Manufacturers are responsible for the ultra-high prices,” argues Krynicki. “They can afford to lower them. The drugs need to be more affordable for people who need obesity care, not just celebrities.”
In a 2024 hearing, Senator Bernie Sanders challenged Novo Nordisk’s CEO on why the same medication costs $969 in the United States but only $59 in Germany – an over 16-fold difference 12. The manufacturer pointed to “significant safety risks” with copycat drugs, praised the FDA for “protecting patients,” and insisted that its $6.5 billion investment this year to expand U.S. production underscores its commitment.
Yet critics remain skeptical that higher supply alone will tame prices, given manufacturers’ inherent profit-seeking incentives. Critics fear manufacturers like Novo Nordisk and Eli Lilly will exploit their temporary monopoly to milk the the GLP-1 cash cow as hard as they can – perpetuating the affordability crisis for patients.
Insurer Incentives: Short-Term Savings
For health insurers, GLP-1 medications pose a thorny financial puzzle. A single patient’s therapy can cost $11,000 or more per year 13 – potentially blowing up budgets if even a modest fraction of eligible members adopt GLP-1 drugs. Now, with the Trump administration reevaluating the Biden administrations decision to require Medicare and Medicaid to cover anti-obesity drugs 14, the stakes could soon escalate.
Insurers are fighting hard against GLP-1 medication coverage for obesity care. AHIP, the largest U.S. health insurer trade group, warns that blanket coverage of weight-loss drugs could “subvert congressional intent” and “bust budgets” if the treatments prove extremely popular 15. Others, like Ceci Connolly of the Alliance of Community Health Plans, argue that “spending big, big bucks on something that still has so many unknowns really jeopardizes the limited dollars and resources that a plan has.” 16
Value to Medicare from Covering and Treating Obesity (Difference from Status Quo)
Yet a 2023 paper from the University of Southern California found that covering weight-loss drugs could save Medicare more than $175 billion to $245 billion over a decade by preventing obesity-related illnesses 17. Dr. Holly Lofton, Director of the Medical Weight Management Program at NYU Langone, emphasizes, “The medications are effective if you can get them – it’s frustrating if you can’t. Insurance access to these meds is the #1 issue in obesity care.”
Part of the problem is what economists call the “turnover problem.” 18 An insurer paying $11,000 for a member’s weight loss this year may never see the payoff if that member switches plans later – a very common occurrence in a society where health insurance is tied to employment and job changes are frequent. This dynamic explains why coverage remains erratic, with companies reluctant to absorb major upfront costs without a guaranteed long-term return.
One former high-ranking insurance executive blames high prices on the underlying profit motive: “insurance companies don’t have a desire for people to be healthier – they make money off people being sick. Doctors fight insurance companies because they actually want people to be well.”
With compounding alternatives disappearing, doctors face a new level of frustration. “Many know how effective GLP-1s can be,” says Dr. Michael Weintraub of NYU Langone’s Endocrinology Department. “But the insurance company is the real gatekeeper. Patients get angry at physicians when they’re denied a known effective tool, and that puts us in a difficult spot.”
Dr. Weintraub’s practice always checks a patient’s insurance beforehand to see if coverage is offered. “More than half of insurers in our area exclude GLP-1 drugs completely,” he notes. Patients shut out of coverage often try suboptimal or risky alternatives, from dubious supplements to black-market medications.
The underlying physiology of obesity also complicates matters. Obesity is a chronic, relapsing condition requiring long-term management. Stopping medication frequently leads to rapid weight regain 19. “Obesity is a chronic condition, and its progressive nature necessitates chronic long-term treatment. If you cease intervention, then the body’s compensatory mechanisms lead to weight regain,” Weintraub explains.
Dr. Marsha Novick, a family physician practicing obesity medicine for 20 years, underscores that “lifestyle changes alone are often not enough for patients with severe obesity. GLP-1s are part of a toolbox that includes meal replacements and even bariatric surgery. Now that they’re more expensive, many patients lose that critical option.”
U.S. Pricing vs. International Models: A Stark Contrast
The FDA ruling also spotlights the vast difference between U.S. and foreign GLP-1 prices. In the U.K., Wegovy (semaglutide 2.4mg) has a list price around $160–$220 per pack, while private pharmacies charge $190–$250 monthly 20 – still far cheaper than the American $1,000-per-month price tag. Countries like France, Australia, and Japan report similarly lower costs. A Yale study found some of the lowest market prices worldwide in places such as China, France, the Philippines, and South Africa 21. Unsurprisingly, the U.S. tops the list of highest GLP-1 prices.
(Source: JAMA Netw Open. 2024;7(3):e243474).
Experts attribute America’s outlier GLP-1 prices to:
Lack of Government Negotiation and Price Controls – Most other wealthy nations have centralized negotiating bodies, forcing manufacturers to accept lower rates or face being excluded from coverage. With rate exceptions, the U.S. government doesn’t negotiate drug prices.
Market Size and Ability to Pay – The U.S. is a high-income market accustomed to elevated drug costs. Companies view American patients as profitable enough to bear steep prices.
Regulatory and Patent Landscape – Other countries may get generic or biosimilar competition earlier, whereas the U.S. remains under patent lock until the early 2030s.
Senator Sanders has lambasted manufacturers for “ripping off Americans with high drug prices,” 22 pointing out that Novo Nordisk reportedly derives 72% of its global GLP-1 revenue from the United States alone 23. Novo Nordisk’s revenue concentration is a staggering imbalance and evidence that Americans are effectively subsidizing global R&D costs by paying inflated prices.
The Economics of GLP-1 Medications: A Fundamental Analysis
The abrupt end to compounded alternatives highlights classic economic principles that shape GLP-1 drug pricing in America:
Monopoly Pricing Under Patent Protection
Patents confer a legal monopoly for 20 years (plus extensions). Without competition, manufacturers can charge far above marginal production cost. Semaglutide, for instance, costs under $5 to produce but sells for $1,000-per-month due to Novo Nordisk’s exclusive commercial rights 24.
Inelastic Demand and Value-Based Pricing
Effective obesity treatments are scarce, making demand relatively inelastic – patients and providers are willing to pay high prices when no close substitutes exist. Companies thus set prices based on the perceived value of weight loss and its health benefits, rather than production costs.
Information Asymmetry and Principal-Agent Problems
Patients often lack full knowledge or direct purchasing power, while physicians, insurers, and pharmaceutical companies each have different incentives. This mismatch leads to inefficiencies in how these drugs are prescribed and reimbursed.
The Third-Party Payer Problem
Instead of direct consumer-vendor transactions, insurance plans decide coverage. With each insurer negotiating separately, pharmaceutical firms face less unified resistance to high prices. Patients, for their part, rarely see the full price – until coverage is denied.
International Price Discrimination
Profit-maximizing firms charge each market according to willingness to pay. Because the U.S. tolerates higher prices, manufacturers capture large profit margins here while accepting lower margins abroad.
Short-Term vs. Long-Term Incentives
Insurers are incentivized to maximize immediate profits rather than investing in longer-term outcomes – they might not reap the benefits if a patient changes plans years later. This undercuts coverage for preventive treatments like GLP-1s, despite potential future savings.
Taken together, these factors create a market failure where monopoly power and fragmented insurance lead to high prices and restricted access – even though society might benefit substantially from widespread, sustainable adoption of these drugs. Ending the compounding workaround removes a modest but meaningful counterweight to the monopoly dynamic, further exacerbating the need for direct policy intervention.
Policy Solutions for a Post-Compounding Era
With the loss of compounded options, policymakers, insurers, and drugmakers face renewed pressure to improve access to GLP-1 medications. Several strategies have increased in urgency:
1. Government Price Negotiation
New provisions from the Inflation Reduction Act give Medicare limited authority to negotiate prices on certain high-cost drugs 25. Over time, GLP-1s could be added to the negotiation list once they meet the statutory requirements. If Medicare – the largest single payer – achieves lower rates, commercial insurers might follow suit or be forced to keep up.
Some officials in the Trump administration have signaled interest in allowing or requiring Medicare and Medicaid to cover anti-obesity drugs 26. If approved, it could create a powerful impetus for price concessions. However, insurers caution that covering such treatments broadly could trigger large immediate expenditures, even if it saves money downstream 27.
2. Insurance Coverage Mandates
The Treat and Reduce Obesity Act (TROA) in Congress aims to let Medicare Part D plans cover weight-loss drugs 28 – a key step toward treating obesity like other chronic diseases. Federal Employee Health Benefits plans have already moved to require coverage of obesity meds, setting a precedent. Mandating coverage in commercial markets, too, could spread costs across the entire pool and make therapy more affordable.
3. Patent and Market Exclusivity Reforms
Reforming patent “evergreening” or expediting biosimilar approvals could bring GLP-1 competition sooner, driving down costs. Evergreening extends monopoly protections through minor tweaks, while “patent thickets” delay generic entry even after core patents expire.
Policy fixes – limiting frivolous patent extensions or fast-tracking biosimilars – face legal and political hurdles but could shorten exclusivity and slash prices 29. Critics note many top-selling drugs remain under overlapping patents far beyond their original terms. Whether these reforms strike the right balance between encouraging innovation and preventing monopolistic abuse remains a key question.
4. March-In Rights
In the most extreme case, march-in rights, authorized under the Bayh-Dole Act, could be used. March-in rights allow the government to license a patent to another manufacturer in extraordinary cases – for instance, if the original patent holder fails to make the invention available on reasonable terms 30. Though rarely used, some advocates argue it could be invoked for GLP-1 drugs if sky-high prices effectively block patient access. Drugmakers counter that such a step would undermine the incentive structure for innovation and likely invite legal battles 31.
5. Alternative Funding and Pricing Models
Outcomes-based contracts – paying only if the drug achieves health improvements – could encourage coverage by reducing the perceived risk 32. States have tested “Netflix” subscription models for hepatitis C treatments, paying a flat rate for unlimited patient access 33. A variant of that approach could theoretically apply to GLP-1s, smoothing out the high per-patient costs.
One intriguing idea is a tiered treatment approach: fully cover expensive GLP-1 therapy for, say, a six-to-twelve-month period to achieve major weight loss, then transition to a cheaper maintenance protocol. This two-phase model addresses insurer anxiety about indefinite high costs while still giving patients a viable path.
A Watershed Moment for Healthcare Access
By declaring that semaglutide and tirzepatide are officially off the shortage list, the FDA has inadvertently exposed the underlying fault lines in American healthcare. Patients who relied on affordable compounded GLP-1s must now confront the branded drug’s steep price tags or risk abandoning a therapy proven to curb obesity and related illnesses.
“GLP-1s work, but the access to care needs to be there,” says Jason Krynicki, summarizing the crux of the crisis. Dr. Holly Lofton echoes this sentiment: “These drugs create hope that weight loss is possible – not as a fad diet, but with better results than old interventions. It’s frustrating that cost so often stands in the way.”
Ultimately, true reform requires more than just improved supply. It demands policy changes – whether through government price negotiation, expanded insurance coverage, or patent reforms – that align the long-term economic gains of preventing chronic disease with the short-term realities of medical decision-making and reimbursement.
As obesity continues to rise, GLP-1 medications represent both a remarkable scientific success and a sobering market failure. The end of compounded alternatives should galvanize stakeholders – from Congress to pharma CEOs – to devise strategies ensuring that life-changing therapies do not remain out of reach for the patients who need them most. Until then, the nation’s GLP-1 affordability crisis remains unresolved, underscoring the urgent need to reconcile innovation with equitable access in American healthcare.
Our Sickcare System May Be Luring GLP-1 Patients into a Health Trap
This is the third of our three-part series on The Ozempic Era. This series explores how the Food Industrial Complex engineered an addiction crisis, how Ozempic emerged as its apparent antidote, and why millions of desperate patients betting their health on GLP-1 drugs may be making a deal with the devil.
The true cost of anti-obesity medications extends far beyond their hefty price tag. Up to one-third of patients’ weight loss comes from lean muscle tissue rather than fat 1, severely impairing their metabolic “furnace.” When treatment ends – whether from patient fatigue, insurance denial, or unmanageable costs – the body is thrown off balance. Patients experience a perfect storm of metabolic maladaptation:
Junk food cravings return with a vengeance,
Diminished muscle mass means a lower resting metabolic rate and reduced calorie burning potential, and
Weight rebounds as their bodies, unable to cope with the sudden excess of junk calories, store this energy as fat.
The toll is brutal: this cycle often leaves patients not only heavier than before but metabolically and psychologically damaged.
Their bodies, having lost critical muscle mass and gained proportionally more fat, are even less equipped to maintain a healthy weight.
Their confidence in medical interventions is shattered.
Their financial resources are depleted.
And perhaps most cruelly, their brief taste of freedom from food addiction makes their return to old patterns all the more painful.
Why are the alluring promises of miracle weight loss drugs failing to manifest for so many patients?
The Terms of the Deal
The Seductive Promise
For eight years, Rachel had tried everything. After her first pregnancy left her struggling with gestational diabetes and stubborn weight gain, she cycled through all the standard interventions: nutritionists, personal trainers, specialized diets. Nothing seemed to touch her body’s newfound resistance to weight loss. Three different primary care physicians dismissed her postpartum weight gain concerns with bland advice about exercise and portion control.
When her doctor finally suggested GLP-1 medication, Rachel spent two months researching before agreeing to start treatment. “There’s so much stigma around these drugs,” she shared with me. Her hesitation reflected a common tension: the desperate desire for change tempered by fear of both the medication’s physical risks and the social implications of relying on pharmaceutical drugs for weight loss.
Nevertheless, the transformation, when it came, was profound. The “food noise” that had plagued her for years – particularly during stressful business travel – simply vanished. Previously irresistible treats became unpalatable. Her longtime love of wine gave way to a complete disinterest in alcohol. The siren song of modern processed foods suddenly seemed to lose its allure.
Millions Scramble to Sign on the Dotted Line
Rachel isn’t alone. Mass media and social media alike are filled to the brim with tales of GLP-1 medications’ unprecedented results: 15-20% 2,3 total body weight reduction, greater impulse control, and – most remarkable of all – a fundamental reset of patients’ relationship with food. Stories like Rachel’s serve as a siren call for the millions of Americans who have endured decades of failed diets and relentless weight regain. These medications promise to restore something they once thought lost: hope.
The emergence of compounded anti-obesity medications, available at a fraction of branded drugs’ costs, has further democratized access to effective weight loss treatments. Over one in eight American adults have now tried these medications 4, an unprecedented adoption rate that speaks to both their effectiveness and the desperation of a population where nearly 75% struggle with excess weight 5.
But beneath the alluring promise of rapid weight loss lies a more complicated reality. As the first wave of patients progresses through treatment, concerning patterns have emerged – patterns that suggest these miracle drugs may extract a steeper price than anyone initially realized.
Read the Fine Print
Most patients view GLP-1 medications as a silver bullet for obesity – just pull the trigger to reclaim your body. And why wouldn’t they hold this belief when they are constantly bombarded with articles 6, advertisements 7, and testimonials 8 touting Ozempic and similar drugs as miracle cures?
Yet the pharmaceutical industry’s position, while quietly stated, is clear: these medications are designed for chronic disease management, not short-term intervention. Just as a diabetic patient requires ongoing insulin treatment, manufacturers maintain that sustained weight management requires continuous GLP-1 treatment 9.
This reality conflicts sharply with both patient expectations and physician hopes. While on the medications, patients experience unprecedented control over their eating habits. This dramatic shift can create an illusion of permanent change, masking the critical need for fundamental lifestyle modifications. Many physicians, observing this positive progress, attempt to wean patients off these medications after reaching their target weights.
But very few patients are prepared for the intensive lifestyle changes needed to maintain their progress once treatment ends. Even patients who understand this need face an unfortunate reality: their treatments are often interrupted before new behaviors can take root.
The result is a system that seems almost intentionally designed for failure: patients begin treatment without understanding the fine print, receive inadequate support during their brief – and expensive – window of opportunity, and very likely face financial or other pressures that force premature discontinuation. This combination of factors transforms what could be an effective strategy for fostering long-term healthy habits into a mere temporary reprieve.
Our Sickcare System Is Failing Patients
The Primary Care Brain Drain
In my recent conversations with physicians, a recurring theme became concerningly evident: physicians are tired. Really really tired.
“Medicine is incredibly stressful – we have the highest suicide rate of any profession,” Dr. Laurie Marbas tells me. After two decades practicing medicine, she’s witnessed the steady erosion of primary care on multiple fronts. Crushing medical school debt drives new doctors toward higher-paying specialties 10, while reduced health insurance reimbursement rates and increased denials put intense financial pressure on patients and physicians alike 11. Doctors often bear the brunt of patient frustrations, increasing burnout risk 12.
Dr. Courtney Younglove, who operates two obesity medicine clinics, describes watching talented colleagues abandon private practice for corporate positions that offer escape from the crushing financial and administrative burden. “Everyone wants out,” she says. The exodus leaves fewer front-line physicians available to manage the growing wave of patients seeking weight loss treatment.
Those who remain face impossible demands:
Profit-driven corporate pressure to see more patients in less time 13 has transformed doctors into “cogs in the wheel,” as one physician bluntly put it to me.
The standard fifteen-minute appointment barely allows time to check vital signs 14, let alone provide the comprehensive lifestyle guidance critical for long-term success on GLP-1s.
Increasingly, health systems plug these gaps with undertrained nurse practitioners who lack the medical expertise to manage complex obesity cases 15.
The Obesity Medicine Training Vacuum
The crisis extends beyond physician availability into the foundations of medical education itself. “I was never taught how to incentivize patients and motivate behavior change. I had to learn that on my own,” Dr. Marbas explains, describing a pervasive gap in obesity medicine training. Medical schools provide virtually no instruction in the complex interplay of nutrition, metabolism, exercise science, and behavioral psychology required for successful long-term weight management 16.
This knowledge gap becomes especially dire when prescribing GLP-1 medications, where the quality of lifestyle support can mean the difference between lasting transformation and devastating relapse. Many physicians lack the expertise to help patients preserve muscle mass during rapid weight loss or navigate the psychological challenges of diet change 17,18. Without this guidance, patients lose their brief window of opportunity for developing sustainable habits before treatment ends.
The problem is systemic: medical education remains focused on treating acute conditions while chronic diseases like obesity require an entirely different skill set 19. As one specialist observed, “We have the best acute care system in the world. If you have an acute medical condition, there’s no better country than America for treatment. We have the most cutting edge medical technology on the planet. But you can’t use an acute care model to treat chronic diseases. Our system is designed for sickcare, not healthcare.”
The Missing Support Infrastructure
Despite billions invested in healthcare technology, the basic infrastructure for successful obesity treatment remains absent: coordinated cross-disciplinary care teams, consistent behavior modification coaching, and proven protocols for managing the critical transition off medication.
The consequences of this infrastructure gap become evident in treatment outcomes. Patient after patient describes receiving their prescription with minimal guidance beyond basic dosing instructions. Critical aspects of treatment – preserving muscle mass, managing side effects, preparing for eventual discontinuation – are left largely unaddressed. The assumption seems to be that the medication alone will somehow solve decades of disordered eating patterns.
And that’s for formal, in-person doctor appointments. Many online compounding GLP-1 sellers merely ask patients to fill out a short intake form in order to receive compounded anti-obesity medications. If patients are lucky, these companies will provide education materials regarding diet change, muscle preservation, and side effects management. But for the vast majority of compounded drug consumers, they are left to fend for themselves – relegated to consultations with Dr. Google or their local weight loss Facebook group.
One may propose that recurring telehealth consultations with medical or nutrition experts are the answer. However, attempts to augment patient care with digital education tools or remote coaching have thus far borne little fruit. “Digital health tools keep getting pitched as the solution,” Dr. Younglove tells me, with an air of mild annoyance. “But they’re just adding complexity without really moving the needle.”
Some weight loss clinics augment their care with lifestyle change coaches. However, many coaches’ strategies rely on the old weight loss playbook of calorie counting and motivation, which runs counter to physicians’ efforts to reframe obesity from an issue of poor willpower to one of biology. The behavioral element of weight loss – understanding trauma, addressing emotional eating, building sustainable habits – often gets lost in the rush to show quick results.
Physicians Are Caught between a Rock and a Hard Place
Healthcare providers face a profound dilemma. They witness the medications’ transformative potential: when patients aren’t constantly battling cravings, when their minds aren’t clouded by intrusive thoughts of food, they finally have the headspace to do the hard work of changing their dietary habits.
However, the protocols physicians know their patients need – comprehensive metabolic monitoring, regular lifestyle counseling, structured transition planning – are often impossible to deliver within the constraints of modern medical practice. Physicians are thus forced to watch as their patients cycle through predictable patterns of initial success followed by devastating relapse.
Some physicians also shared with me in private a growing frustration of the quick-fix mindset held by many GLP-1-seeking patients. Doctors increasingly find themselves cast as gatekeepers to medication rather than partners in health transformation.
As trust erodes between patients and providers, the fundamental doctor-patient relationship suffers. Our sickcare system’s failure to support preventative care or lifestyle change mutates what should be a healing partnership into an adversarial dynamic centered around prescription access.
Uncovering Ozempic’s Physiological Traps
During Treatment: Deteriorating Body Composition
When patients begin GLP-1 treatment, few understand the hidden cost to their body’s fundamental architecture. A substantial portion of patient’s weight loss comes not from fat but from lean body mass 20, which consists of muscles, bones, organs, skin, and other non-fat components.
The loss of muscle mass creates changes in body composition that lead to accelerated biological aging, setting up conditions for a cascade of metabolic complications 21. Studies also show significant reductions in bone mineral density, which is particularly concerning for premenopausal women 22.
“For all weight loss, you’re losing both fat and muscle,” explains S.M., a dietitian who has spent her career working with eating disorders. “But when you regain weight, it comes back primarily as fat unless you’ve maintained adequate protein intake and resistance training throughout treatment.”
This asymmetric pattern of fat + muscle loss followed by fat regain progressively erodes patients’ lean mass. Even if patients successfully achieve their target body weight, they may experience “skinny fat” syndrome – a form of metabolic obesity where their normal weight masks a high body fat percentage and dangerous metabolic dysfunction 23.
The physician oversight gap compounds these challenges. Many prescribers – particularly online providers – provide little information about avoiding muscle loss. Without proper guidance on nutrition and exercise during treatment, patients unknowingly sacrifice the very tissue they need most for health and longevity. More troubling still, this deterioration occurs silently, masked by the euphoria of watching the numbers on the scale decrease.
Post-Treatment: Metabolic Dysfunction
The consequences of muscle loss extend far beyond aesthetics into the realm of fundamental metabolic health. As metabolically active tissue diminishes, patients experience a permanent reduction in their resting metabolic rate 24 – the calories burned while at rest. But this direct impact of muscle loss tells only part of the story.
The body, interpreting rapid weight loss as a sign of starvation, initiates a complex hormonal cascade that fundamentally alters how it processes and stores energy:
This hormonal rebellion begins with leptin, the body’s primary satiety hormone. As fat tissue decreases, leptin levels plummet 25.
Calorie restriction leads to increased production of ghrelin – the hormone responsible for hunger signaling 26.
Simultaneously, the body becomes more sensitive to neuropeptide Y, a powerful stimulator of appetite and fat storage 27.
“When people lose weight, their bodies treat it like starvation,” S.M. explains. “The body lives compensates by requiring fewer calories to maintain basic functions.” This metabolic adaptation persists even after weight regain, creating a perfect storm of increased hunger, reduced calorie burning, and enhanced fat storage. These changes leaving patients fighting not just their habits but their own biology.
This disruption extends to core metabolic systems, affecting everything from glucose metabolism to insulin sensitivity 28. Even while maintaining their target weight on medication, patients often show elevated inflammatory markers and disrupted cortisol patterns 29 that encourage abdominal fat storage 30. Without proper medical oversight, these changes can seriously harm a patient’s metabolism – a cruel irony for those who paid an exorbitant price to improve their health.
Post-Treatment: Weight Rebound – Mostly Fat
When treatment ends – whether from side effects, cost, or insurance denial – the body’s response is swift and devastating. Patients report what S.M. describes as “insatiable hunger,” wherein cravings return with unprecedented intensity 31 – particularly for high-carb, calorie-dense junk foods. “The food chatter returns – that’s what patients find most distressing,” explains Dr. Francavilla Brown.
Patients’ bodies, primed by months of restricted eating and a diminished metabolism, aggressively store this flood of calories as fat rather than rebuilding lost muscle tissue. While some patients maintain their progress through older, more affordable – and less effective – weight loss medications, many experience rapid weight rebound. The weight regain is particularly severe for those with insulin resistance who return to high-glycemic foods after ceasing treatment.
Patients regain on average two-thirds of their lost weight after ceasing GLP-1 treatment, often in the form of increased central adiposity. “If someone has lost 40 pounds but 15-20 pounds were muscle, the weight regained is most likely fat,” Dr. Francavilla Brown informs me. “And they’re likely worse off metabolically than if they’d never started the medications in the first place.”
This preferential storage of regained weight around the abdomen 32 carries particular health consequences, including increased risk of heart disease, stroke, type 2 diabetes, insulin resistance, and other cardiovascular and metabolic disorders 33.
Long-Term Consequences: Weight Cycling
When patients rapidly lose a significant amount of weight – whether naturally or with medication – more than half of the lost weight returns within two years. By five years, more than 80% is regained 34. This treatment discontinuation puts patients’ health in severe jeopardy.
This pattern of rapid loss and eventual regain appears to be accelerating the onset of chronic disease 35. The implications become particularly clear in examining metabolic health markers 36. Studies show that individuals who maintain stable weights, even if elevated, often demonstrate better biomarkers than those who cycle through periods of loss and regain 37. A 2022 study found that the number and degree of weight cycles were positively associated with increased risk of type 2 diabetes and hypertension, particularly among women and individuals with normal BMI 38.
More concerning still, recent research has challenged long-held assumptions about who faces the greatest risks. While weight cycling’s negative effects were historically thought most relevant to geriatric or normal-weight populations, new evidence suggests these impacts may be even more severe in individuals with obesity 39. These findings suggest that our current approach to obesity treatment may be creating a new category of patients with complex, treatment-resistant conditions that manifest decades earlier than in the general population 40.
It’s Time to Renegotiate the Deal
The Devil’s in the Details
The toll of treatment disruption extends far beyond metabolic damage. Dr. Younglove describes watching patients disappear from care entirely after discontinuing treatment, their brief taste of freedom from food addiction giving way to a sense of shame and resignation. This pattern of treatment abandonment leads to a broader concern: patients who attempt and fail GLP-1 therapy may become dejected and lose faith in the medical system.
The financial toll compounds this psychological burden. While systematic studies of the economic impact are still emerging, early analyses suggest that GLP-1 drug costs vastly exceed any potential long-term healthcare savings 41 – mostly due to premature treatment discontinuation. This calculation doesn’t account for the financial and emotional anxiety many patients experience during treatment, often depleting savings or incurring substantial debt just to maintain drug access.
This combination of factors – psychological trauma, financial strain, and post-treatment medical complications – transforms what could be a powerful therapeutic tool into a dangerous game of chance for their long-term health. As CRC Group’s analysis concluded, “If an untrained clinician prescribes GLP-1s without appropriate support, an individual could actually become sicker.” 42
The promise of pharmaceutical intervention means little without the systems necessary to foster lasting change. The medical community now faces an urgent question: how can they meet patients’ urgent weight loss needs without putting their long-term metabolic health at risk?
The Bill Is Coming Due
Insurers Pulling Coverage
A financial crisis looms over the GLP-1 treatment landscape. And our broken health insurance system is exacerbating these challenges:
Major insurers are increasingly implementing coverage exclusions, arbitrary BMI thresholds, and strict treatment time limits that all but guarantee treatment disruption 43.
Some private insurers 44 have implemented sweeping obesity coverage exclusions, often citing poor patient adherence 45.
Medicare’s continued prohibition of anti-obesity medication coverage 46 gives private insurers permission to follow suit.
State health plans like Colorado’s 47 and West Virgina’s 48 are moving to eliminate coverage for obesity treatment.
The pattern proves particularly devastating when insurers revoke existing coverage. “Some insurance plans will cover medication for weight loss,” Dr. Francavilla Brown explains, “but after a year or two will decide it’s not cost effective and stop covering it.” This rug pull leaves presents patients with a hard choice: deplete their savings to maintain treatment or discontinue the medications and put their health in jeopardy.
No More Cheap Ozempic
Concurrently, the FDA’s recent decision to declare the tirzepatide (and soon semaglutide) shortage over will imminently eliminate access to affordable compounded versions of weight loss medications drugs 49. While this may be a win for patient safety 50, the timing couldn’t be worse.
The FDA’s regulatory shift comes just as online prescribing services have reached a critical mass. Millions of patients have come to rely on compounded medications for obesity treatment 51, thanks in part to the loose prescribing practices of digital health companies 52.
These companies, which are operating in a regulatory grey zone and were quick to capitalize on the compounding loophole, typically lack contingency plans for patients who can’t afford branded medications or face treatment disruption. “It’s a concern with mass prescribing companies,” Dr. Francavilla Brown notes. “If cheap compounded medications go away, what other options can you provide patients if you’re a one-trick pony?”
Reimagining Obesity Care: Calls for Systemic Change
The rise of GLP-1 medications represents both a breakthrough and a warning. While these drugs have demonstrated unprecedented effectiveness in treating obesity, their implementation reveals fundamental flaws in America’s approach to chronic disease management.
The current system, built around short-term interventions and quarterly profit reports, systematically undermines patient health through fragmented care, arbitrary coverage restrictions, and inadequate support infrastructure.
Dr. Laurie Marbas’ Recommendations
Creating sustainable solutions requires a complete reimagining of obesity care. Dr. Laurie Marbas, who has spent 20 years in medicine and 8 years specializing in lifestyle medicine, suggests that sustainable change requires addressing both medical education and patient behavior.
First, medical training must evolve. Dr. Marbas shared her belief that physicians need training not just in prescribing medications, but in health psychology and behavior change. Incorporating lifestyle medicine into medical school curricula and board certification requirements would help prepare doctors to support lasting transformation.
Dr. Marbas also proposes employer-facing programs to orient consumers away from ultra-processed foods and towards more healthful, whole foods. She points to programs like Plantstrong and Metabite, which partner with self-insured employers to implement comprehensive lifestyle changes.
Dr. Marbas states these programs have achieved 5-9% body weight reductions through plant-inclusive diets while improving blood sugar and cholesterol levels. Crucially, their payment models align incentives with outcomes – they only get paid by employers when patients achieve specific health improvements.
Dr. Carolynn Francavilla Brown’s Recommendations
Dr. Carolynn Francavilla Brown’s practice offers another model for comprehensive care. Her clinic offers:
Regular body composition testing to monitor muscle mass preservation.
Specific, customized protein and exercise targets.
Ongoing lifestyle counseling.
This detailed monitoring helps prevent severe muscle loss, which is critical for long-term weight loss success.
The financial barriers to treatment also require systemic reform. Dr. Francavilla Brown notes that while insurance coverage for GLP-1 drugs remains wildly inconsistent, more stable treatment options exist. She points out that bariatric surgery, while more invasive, also tends to be more effective and durable. The procedure is also more affordable than GLP-1 medications due to wider, more consistent insurance coverage.
Dr. Courtney Younglove’s Recommendations
Dr. Younglove’s experience with employer-based solutions offers one promising path forward. She proposes a comprehensive model combining:
Obesity medicine protocols,
Clinical teams trained to handle basic care with experts available for consultation for complex cases, and
Dedicated behavioral health support.
This integrated approach acknowledges that sustainable weight loss requires addressing both physical and psychological factors.
Digital health tools, while fashionable, often add complexity without improving outcomes. “A lot of people throw money at easy things that don’t move the needle,” Dr. Younglove notes. Her clinics’ experiments with digital education platforms revealed low patient engagement, suggesting technology alone cannot drive behavioral change.
Upstream policy changes may offer the most leverage. “We need vegetables to be cheaper, not more expensive,” Younglove emphasizes. This requires policy intervention to realign food subsidies and market incentives toward promoting metabolic health.
The Path Forward
The story of GLP-1 medications reveals a healthcare system at a crossroads. These drugs have delivered life-changing weight loss for countless Americans but at a steep price: metabolic strain, soaring costs, and a healthcare system unprepared to provide meaningful long-term support.
It’s time for patients, providers, and policymakers to demand a healthcare system that treats obesity as the chronic disease it is – not as a series of quick fixes doomed by short-sighted insurance policies and profit-driven prescriptions:
Reforming health insurance to ensure obesity treatment is covered the same as that for any chronic disease
Pushing for transparent drug pricing from insurers and manufacturers
Integrating behavioral health and nutrition specialist support with medical care to promote sustainable behavior change rather than only short-term results
Putting greater emphasis on obesity care and lifestyle medicine practices into standard medical education
Implementing upstream policy changes that make healthy food and lifestyle choices more economically accessible
Comprehensive medical monitoring of body composition and metabolic health
The challenges are significant, but the consequences of not acting are dire. By learning from these models and implementing systemic changes, we can build a healthcare system truly capable of supporting lasting transformation in patients’ lives.
GLP-1 Drugs Have Emerged as a Panacea for Addiction – If You Can Afford Them
This is the second of our three-part series on The Ozempic Era. This series explores how the Food Industrial Complex engineered an addiction crisis, how Ozempic emerged as its apparent antidote, and why millions of desperate patients betting their health on GLP-1 drugs may be making a deal with the devil.
The Rise of Ozempic: Medicine’s New “Silver Bullet“
The story of how GLP-1 agonists transformed from diabetes medication to potential addiction panacea begins, like many medical breakthroughs, with an unexpected observation and a Eureka moment.
Eureka! Discovering the Miracle Drug
Ozempic’s story begins in the labs of researchers seeking to better manage type 2 diabetes. Clinicians began to notice that diabetes patients taking semaglutide – a peptide drug sold by Novo Nordisk under the brand name Ozempic – weren’t just achieving better blood sugar control 1. They were shedding significant amounts of weight. Not the modest few pounds traditionally seen with other diabetes medications, but dramatic losses of 15% or more of their total body weight 2.
What made this weight loss different was its consistency. Previous weight loss medications had modestly helped some patients dramatically while doing virtually nothing for others. But semaglutide delivered significant results across broad populations.
More importantly, patients described a profound shift in their relationship with food. The constant cravings, the intrusive thoughts about eating, the loss of control around certain hyperpalatable foods – these hallmarks of food addiction began to fade. For the first time, physicians had a tool that seemed powerful enough to counter the biochemical trickery of engineered “craveware” foods.
Figure: GLP-1 research and commercial milestones, 1978-2022 3
A Solution to Addictive “Craveware”
At Ozempic’s core is semaglutide, a synthetic version of a naturally occurring hormone called GLP-1 (glucagon-like peptide-1) that is typically administered once a week via a subcutaneous injection. The body naturally releases GLP-1 after meals to regulate and protect the body. Semaglutide supercharges that process: by binding to GLP-1 receptors in the pancreas, brain, and stomach, semaglutide slows gastric emptying, reduces appetite through direct action on brain centers, improves insulin sensitivity, and – most intriguingly – appears to modulate the very reward circuits that make hyperpalatable foods so irresistible 4.
Yet the drug’s wide-ranging impact doesn’t stop at waistlines. As more data emerged, researchers began noticing something even more remarkable: GLP-1 drugs appear to slow neurodegenerative diseases 5 and curb addiction-related behaviors beyond just food 6. Early studies suggested potential benefits for alcohol cravings, nicotine dependence, and other compulsive behaviors. The implications were profound: had we stumbled upon a master key to human cravings?
The Weight Loss Drug Gold Rush
Once word got out that a “miracle shot” could slash body weight by double digits, demand exploded. By early 2024, approximately one in eight American adults reported having taken a GLP-1 agonist 7. Novo Nordisk, the Danish pharmaceutical giant behind Ozempic and Wegovy, saw a massive revenue surge and became Europe’s most valuable company 8. Competitors hustled to keep pace.
The FDA’s GLP-1 agonist approval timeline reveals the frenzied pace of the weight loss medication gold rush:
Year Approved
Brand Name
Drug Component
Company
Approved Use
2005
Byetta
Exenatide
AstraZeneca
Type 2 diabetes
2010
Victoza
Liraglutide
Novo Nordisk
Type 2 diabetes
2014
Saxenda
Liraglutide
Novo Nordisk
Chronic weight management
2017
Ozempic
Semaglutide
Novo Nordisk
Type 2 diabetes
2019
Rybelsus
Semaglutide
Novo Nordisk
Type 2 diabetes
2021
Wegovy
Semaglutide
Novo Nordisk
Chronic weight management
2022
Mounjaro
Tirzepatide
Eli Lilly
Type 2 diabetes
2023
Zepbound
Tirzepatide
Eli Lilly
Chronic weight management
Eli Lilly wasn’t far behind. Eli Lilly’s tirzepatide (Mounjaro/Zepbound) added a second mechanism of action, targeting both GLP-1 and GIP (gastric inhibitory polypeptide) receptors 9. The weight loss results approached bariatric surgery territory – up to 20% total body weight loss in clinical trials 10 – but without permanent anatomical alterations.
While tirzepatide patients have been slimming down, Eli Lilly has been fattening up: Eli Lilly’s valuation has tripled to nearly $1 trillion 11, eclipsing Novo Nordisk’s early dominance and catapulting it to the top of list of world’s most valuable healthcare companies 12.
The broader pharmaceutical industry has taken notice. Tirzepatide and semaglutide are currently considered the most effective medications for weight loss 14, but at least 16 new obesity drugs are anticipated to enter the market in the next five years 15. Companies including Roche, Amgen, Pfizer, and AstraZeneca are all racing to claim their share of what promises to be a $100+ billion market.
Is Ozempic Too Good to Be True?
The medical community’s excitement is understandable. For decades, we’d fought the obesity epidemic with tools that seemed hopelessly mismatched against the sophisticated engineering of modern processed foods. Now, at long last, we have a pharmaceutical intervention that can potentially disrupt the very reward pathways that make industrially engineered foods so addictive.
Ozempic’s Physical Toll
The first signs of trouble appeared in the routine follow-up visits. Patients reported dramatic weight loss success, yes, but something else was happening to their bodies. Physicians began noticing troubling gastrointestinal symptoms and changes in body composition.
The gastrointestinal side effects have been well documented: nausea, vomiting, and constipation so severe that they rank among the top reasons for patient discontinuing GLP-1 medications 16. And yet, these immediate discomforts may prove less significant than the longer-term changes happening beneath the surface.
Recent research has revealed that up to one-third of the weight lost on GLP-1 medications comes from lean muscle mass rather than fat 17. This isn’t just a cosmetic concern. The gradual loss of muscle mass and strength can lead to a cascade of negative health outcomes: lower metabolic rates, reduced functional capacity, and an increased risk of developing what researchers call “skinny fat” syndrome – normal weight but metabolically unhealthy 18.
“My biggest concern with GLP-1s is that they may be too effective,” one obesity medicine specialist with nearly two decades of primary care experience shared with me. “These drugs can completely eliminate appropriate hunger, which is a normal and necessary human phenomenon. If patients are happy without eating, that’s dangerous – they lose lean mass.” Some physicians are now finding that in certain cases, it may be better for patients to remain overweight but preserve muscle mass than to achieve dramatic weight loss at the expense of lean tissue.
Some patients have also reported dramatic changes in facial aging, dubbed “Ozempic face” in the media 19. While this might seem superficial compared to the aforementioned medical concerns, unwanted changes in face composition can take a major psychological toll. More concerningly, these surface-level changes hint at a broader pattern of rapid physiological changes caused by Ozempic that have profound consequences for health and aging. More on this in Part III.
Ozempic Helps Weight Loss, but It’s Not an Obesity Cure
The drugs work. The weight comes off. Patients report reduced cravings and improved control over their appetites. “These medications create mental headspace,” one obesity medicine specialist with nearly two decades of clinical experience explained to me. “When you’re not constantly battling cravings, when your brain isn’t overwhelmed with intrusive thoughts about food, you finally have the capacity to do the hard work of changing your relationship with eating.”
Hard work is the opposite of a silver bullet. This window of opportunity – this period of reduced cravings and increased control – represents a crucial chance for patients to establish new habits and behaviors. But here’s the critical caveat: GLP-1 drugs aren’t an obesity cure. They only control cravings and addictions while actively taking them. Unless patients use this window to fundamentally change their lifestyle and relationship with food, the cravings will return with a vengeance as soon as they stop the medication.
This caveat transforms GLP-1 drugs from a miracle cure to a maintenance medication. In the worst-case scenario, they’re a life sentence. Like insulin for diabetes or antidepressants for depression, they become part of a long-term strategy for managing chronic disease. “We need to shift our understanding of obesity,” argues another obesity medicine specialist. “This isn’t about willpower or short-term fixes. It’s a chronic disease that requires ongoing treatment, just like hypertension or diabetes.”
But this is where the promise of GLP-1 drugs collides with the harsh realities of American healthcare. The support infrastructure needed to help patients make lasting changes – the behavioral health resources, the nutritional counseling, the coordinated care teams – is largely missing.
The Health System Isn’t Ready for Weight Loss Patients
Beyond the physical side effects, our healthcare system is fundamentally unprepared to manage patients on these medications. The data is clear: GLP-1 patients have the greatest success with high-touch, coordinated care that combines medication management with lifestyle interventions 20. Yet our primary care infrastructure isn’t built to deliver this level of support.
Primary care physicians (PCPs) are poorly equipped for the kind of high-touch health management required to successfully navigate the weight loss journey 21:
Low bandwidth: Primary care providers often lack the bandwidth to offer the intense patient engagement and support needed for healthy, lasting weight loss. Initiating, titrating, and monitoring GLP-1 drugs significantly adds to PCP workloads. And it takes a lot of time and effort to help patients navigate the drug’s side effects and required lifestyle modifications.
Inexperienced: Medical professionals often lack experience in obesity management. Primary care providers aren’t necessarily fully aware of the comprehensive care required, from addressing nutritional biochemistry to understanding mitochondrial dysfunction.
Poorly resourced: Many PCPs lack the resources necessary for proper patient screening and monitoring. PCPs and clinics also often don’t have access to the multidisciplinary care teams – diabetes care specialists, bariatric health care providers, dietitians, nutritionists – needed for comprehensive obesity management. They are also unable to provide adequate coaching on nutrition and exercise practices to improve weight loss outcomes while on the drug.
The result? Many patients receive prescriptions without the comprehensive support system needed for long-term success 22. They’re left to navigate severe side effects, complex lifestyle changes, and critical nutritional needs largely on their own. Often this leads to a failure to modify consumption behaviors, discontinuation of treatment, and rapid weight regain.
The Dark Side of Ozempic: Treatment Roulette
The stark reality of GLP-1 drugs emerges in a single devastating statistic: only 15% of U.S. patients prescribed GLP-1 drugs for weight loss continue treatment after two years 23. This bleak adherence figure should horrify anyone concerned with public health and solving the obesity crisis.
These drugs aren’t just another diet pill – they represent our best tool yet for treating food addiction. But this treatment only works with sustained access and support. Those conditions are proving to be a very tall order for the American healthcare system.
Weight Loss Drugs’ Pervasive Supply Shortages
Ozempic’s success brought its own complications. From day one, Wegovy and Zepbound – Novo’s and Lilly’s respective weight loss medications – have been in critically short supply. Manufacturing has consistently struggled to keep pace with skyrocketing demand, creating a chaotic landscape where diabetes patients find themselves competing with weight loss seekers for limited supplies of Ozempic and Monjouro, which are intended for diabetes management 24.
Healthcare providers have spent multiple years grappling with unreliable availability, forcing healthcare providers into impossible choices about patient prioritization. “Semaglutide and tirzepatide supply issues were a significant problem [in 2024],” emphasizes Dr. Laura Davisson, Professor of Medicine and Director of Medical Weight Management at West Virginia University. “Not every patient who needs to lose weight needs a GLP-1, but obesity medicine specialists should be able to make [treatment] decisions based on medical reasons.”
Weight Loss Drugs’ Onerous Financial Burden
Supply is only half the problem. The other half is price. The cost burden of Ozempic on patients is staggering. With a price tag of over $12,000 per year, most patients face difficult choices about starting or continuing treatment.
Despite the drugs’ significant weight-loss efficacy, the ongoing financial burden makes GLP-1 drugs inaccessible for many – particularly for uninsured or underinsured populations. A recent study found that 54% of people on GLP-1 drugs reported difficulty managing the cost, including 22% who described it as “very difficult.” Even among insured users, 53% struggled with affordability 25.
A comprehensive analysis revealed that individuals without diabetes who began GLP-1 drugs for obesity saw their healthcare costs increase by $4,206 in their second year compared to those not on GLP-1 therapy. Contrary to popular expectation, weight loss drugs did not lead to a reduction in obesity-related medical episode (e.g. diabetes, cardiovascular disease) costs 26.
This dramatic increase in net cost of care – the costs of GLP-1 therapy minus savings due to reduced obesity-related medical issues – for obesity treatment raises serious questions about the long-term cost-effectiveness of these treatments for both individual patients and the healthcare system as a whole.
Health Insurers Beat a Hasty Retreat
Most employer plans limit or exclude coverage of weight loss medications, leaving many to pay out-of-pocket 27. “Access is currently being decided based on whether these medications are included in someone’s plan,” Dr. Davisson continues. “[Even] if the medications are on someone’s plan, extremely variable sets of restrictions are being placed on access. The hoops a patient has to jump through are inconsistent between every different plan.”
In response to supply and cost pressures, several major insurance companies are dropping the pretense and are entirely eliminating coverage of these medications for obesity 28. ACA Marketplace plans limit GLP-1 drug coverage to patients with chronic diseases like diabetes 29. Medicare prohibits coverage of anti-obesity medications unless used to treat other conditions, such as type 2 diabetes or cardiovascular disease.
Such carveouts would be unthinkable for almost any other chronic disease. But the message is clear: obesity treatment remains categorized as cosmetic or lifestyle-related rather than medically necessary, despite overwhelming evidence to the contrary. These coverage exclusions ignore the chronic disease nature of obesity and ignore the complex relationship between obesity and metabolic conditions such as diabetes.
Treatment Roulette
These supply shortages and insurance coverage restrictions are increasingly placing the brunt of the psychological and financial burden on medically uneducated, socioeconomically disadvantaged portions of the population. For patients, this often results in playing a dangerous game of treatment roulette – never knowing if their next prescription will be filled.
These treatment interruptions aren’t just inconvenient; they undo months of weight loss progress and jeopardize patients’ health. When treatment stops abruptly, patients often experience rapid weight regain along with the return of the food cravings and behavioral patterns they had worked so hard to overcome.
Temporary Relief: The Era of Cheap Compounded GLP-1s
As millions of Americans face the harsh realities of drug access barriers, a shadow healthcare system has emerged to fill the gap. Millions of patients, priced out of Ozempic and desperate to maintain their weight loss progress, turned to compounding pharmacies that offer generic versions of weight loss medications at a fraction of the cost. Compounding pharmacies, once a niche player in pharmaceutical manufacturing, have become an essential lifeline for patients desperate to maintain their weight loss treatment.
GLP-1 Compounders Fill the Gap
The appeal of compounded GLP-1 drugs is immediately obvious: while branded GLP-1s cost upwards of $1,300 monthly, compounded versions typically run $300-400. For the majority of patients struggling with insurance denials or prohibitive copays, this price difference is the difference between continuing treatment and being forced to stop.
But cost savings are only part of the story. When supply chain chaos left pharmacy shelves empty of brand-name Ozempic, Wegovy, Mounjaro, and Zepbound, compounding pharmacies kept patients on therapy who would otherwise have faced dangerous treatment interruptions 30.
Under FDA emergency rules, official compounding facilities can legally gain authorization to produce medications during officially declared shortages. The FDA declared a semaglutide shortage in March 2022 and tirzepatide shortage in December 2022 31.
The process of drug compounding appears at first glance relatively straightforward: pharmacists combine pharmaceutical ingredients to create versions of semaglutide or tirzepatide that mirror the active components of branded drugs. While not identical to the originals, these compounded versions offered a viable alternative for many patients.
The numbers tell the story: an estimated 30% of GLP-1 users in the United States have obtained their medication from compounding pharmacies 32. That’s potentially millions of Americans who found a path to continued treatment through this alternative channel.
Pharma Giants Raise the Alarm
The pharmaceutical giants didn’t welcome the competition. Novo Nordisk and Eli Lilly launched aggressive campaigns questioning the safety and consistency of compounded medications. Their argument centered on quality control: because compounded drugs don’t undergo the FDA’s standard review process, they claimed, variations in purity, potency, or sterility could put patients at risk 33.
Many obesity advocacy organizations and specialists have aligned with this position, refusing to work with compounded versions entirely. “Patient safety comes first,” explains Dr. Maribeth Orr, a board-certified Obesity Medicine physician at Heartland Weight Loss. “While we want nothing more than for patients to get treatment, we can’t support something so unregulated and risky.”
Compounding pharmacies and their supporters argue that these concerns are overblown, pointing to their long history of safely producing numerous other medications and their adherence to strict quality control standards. They see a different motivation behind Big Pharma’s opposition 34: with GLP-1 medications projected to become a $100+ billion market, pharmaceutical companies have an obvious interest in maintaining their oligopoly and pricing power. The existence of much cheaper compounded alternatives threatens their profit potential 35.
The pharmaceutical companies haven’t limited their response to public relations. They’ve backed their safety concerns with legal muscle, filing lawsuits and lobbying intensively to restrict compounding. Eli Lilly, in particular, has taken an aggressive stance against sellers of compounded tirzepatide versions 36.
The safety of legal compounded medications remains contested. While official compounding pharmacies are required by the FDA to follow strict protocols, they indeed don’t face the same rigorous oversight as large pharmaceutical manufacturers. Furthermore, the FDA has received numerous safety complaints about certain compounded GLP-1 formulations, underscoring this risk 37. And beyond legal compounders, dark market GLP-1 drug sellers operate with no regulatory oversight, posing severe health and legal risks for consumers 38.
However, for many patients desperately seeking treatment, the choice isn’t between branded and compounded medications – it’s between compounded medications and no treatment at all 39. When framed in these terms, the decision for many is simple.
The Rug Pull: FDA Declares the Shortage Over
For a moment, it seemed that off-label use and compounding might offer a supply and cost solution for patients, helping to maintain drug access. Patients facing treatment disruption due to supply shortages had an alternative source. The existence of this parallel market even creates some pressure on pharmaceutical companies to reconsider their pricing strategies 40.
But now some patients’ window of hope is rapidly closing. The FDA has declared the tirzepatide shortage over, and semaglutide will quickly follow suit, portending doom for the GLP-1 compounding market 41. This declaration leaves vulnerable patients with an impossible choice: pay thousands for name brand medications or stop treatment altogether. Millions more patients may join the 85% of people who discontinue weight loss treatment within two years.
The consequences of this mass discontinuation may prove catastrophic. As we’ll explore in Part III, there’s growing evidence that prematurely disrupting GLP-1 treatment can have severe negative physiological consequences.
When the dust settles, America’s experiment with GLP-1 drugs may prove to have been a deal with the devil: attracting millions with the unprecedented hope of curing food addiction and obesity, only to leave patients worse off – financially, physically, and psychologically – than ever before.
How Tobacco Giants Hacked Hunger and Broke Our Bodies
This is the first of our three-part series on The Ozempic Era. This series explores how the Food Industrial Complex engineered an addiction crisis, how Ozempic emerged as its apparent antidote, and why millions of desperate patients betting their health on GLP-1 drugs may be making a deal with the devil.
The Great Transformation: Obesity Consumes the World
The statistics tell one story. The old photos tell another. Look through family albums from the 1950s or early ’60s, and you’ll see a different America. Beach photos, graduation ceremonies, family picnics – the people look almost impossibly lean by today’s standards. This wasn’t just aesthetics; it was the norm. In 1960, just 13% of American adults were classified as obese 1. Today, that figure seems unfathomable.
The Old Regime: When Malnutrition Was Public Enemy #1
Prior to the 1970s, malnutrition and undernourishment remained more pressing issues in many parts of the world: my maternal grandmother, who grew up in an orphanage under extreme poverty, developed rickets from malnutrition – a condition virtually unknown in America today 2. Her generation’s healthcare providers were far more preoccupied with battling diseases of deprivation – rickets, pellagra, and other nutritional deficiencies that now appear primarily in medical textbooks – rather than counting calories.
It wasn’t just about food availability. Daily life itself demanded more movement. Agricultural and factory labor dominated the workforce. Most households had a single car, if any. Suburban sprawl hadn’t yet reshaped our cities into unwalkable expanses. And perhaps most crucially, processed foods were the exception rather than the rule – most meals were cooked at home using fresh or minimally processed ingredients.
It wasn’t a golden age by any stretch of the imagination – food inequality and undernourishment remained a grim reality in parts of the U.S. and abroad. But on the whole, widespread overconsumption of calories wasn’t yet embedded into every corner of daily life.
Brave New World: Post-1970s
The transformation began quietly in the mid-1970s. At first, the uptick in obesity rates seemed like a statistical blip. But by the early 1980s, the trend was unmistakable: across every race, age, and gender, Americans were packing on the pounds – and fast 3. Obesity rates jumped from 13% obesity in 1960 to over 40% today 4. The U.S. now has some of the highest obesity rates in the world – over three-quarters of adults are overweight or obese 5.
Figure: Share of adults that are obese, 1975 to 2016 6
While America led this transformation, it didn’t remain an American phenomenon for long. The obesity epidemic has gone fully global, spreading first to other affluent Western nations, then to emerging economies such as China or Saudi Arabia, and now to developing nations across the global south.
Today’s numbers paint a startling picture of this global transformation: 43% of adults worldwide – over 2.5 billion people – are now considered overweight. 16% of the global adult population is classified as obese 7. Nations that once battled undernourishment now face an onslaught of fast-food chains, sugar-sweetened beverages, and shelf-stable snacks high in fat and salt.
Craveware: How the Food Industrial Complex Hacked Hunger
The conventional narrative blames the obesity epidemic on a simple calories-in, calories-out equation gone wrong. But that explanation misses the orchestrated campaign that reshaped global eating habits.
The true inflection point came in the 1980s, when major tobacco companies, facing declining cigarette sales and mounting public health concerns, began acquiring food manufacturers en masse: Philip Morris purchased General Foods in 1985 and Kraft in 1988, while R.J. Reynolds acquired Nabisco in 1985 8. These weren’t just diversification plays. The tobacco giants brought something far more valuable than capital to their new food subsidiaries: decades of expertise in creating dependency by engineering and marketing addictive products.
The results were transformative. Under tobacco company ownership, food products became dramatically more “hyperpalatable” – industry speak for engineered combinations of fats, sugars, and sodium not found in nature that trigger compulsive consumption 9. Recent research reveals the scope of this transformation: Foods owned by tobacco companies were 80% more likely to contain potent combinations of carbs and sodium and were 29% more likely to contain powerful combinations of fats and sodium 10. Today, a staggering 68% of the American food supply meets the scientific criteria for hyperpalatability 11.
This isn’t just processed food; it’s addiction engineering. The same companies that spent decades optimizing nicotine delivery systems turned their expertise to engineering foods that override natural satiety signals and hijack reward pathways in the brain. These addictive combos serve as “craveware” that hacks our brain’s reward center, enticing us to eat beyond satiety – exactly what corporate bottom lines demand. Add an onslaught of marketing campaigns and “value meals” that stack cheap calories high, and you have a perfect recipe for widespread obesity 12.
The Health Reckoning for Obesity
The consequences of this transformation extend far beyond aesthetics or clothing sizes. The medical community now finds itself battling a cascade of obesity-related health conditions that threaten to overwhelm healthcare systems globally:
Cardiovascular Diseases
• Each 5-point increase in BMI corresponds to a 27% higher risk of coronary heart disease and an 18% increased risk of stroke 13.
• Hypertension rates jump from 24% in normal-weight individuals to 54% in those with BMI ≥35 14.
Metabolic Disorders
• Up to 70% of patients with obesity develop dyslipidemia 15.
• Type 2 diabetes risk increases dramatically with BMI 16.
• Non-alcoholic fatty liver disease (NAFLD) has become endemic in obese populations 17.
Cancer
• Obesity is now recognized as a major risk factor for multiple cancers, including esophageal, colon, liver, pancreatic, and kidney malignancies 18.
• The inflammation associated with obesity creates an internal environment that promotes tumor growth and progression
• Obesity can impact fertility and increase complications during pregnancy 20.
• Obesity is linked to increased all-cause mortality, with the risk increasing as BMI rises 21.
What we’re witnessing isn’t just a public health crisis – it’s the largest transformation of human bodies in recorded history. And unlike infectious diseases or natural disasters, this epidemic was intentionally engineered, marketed, and sold to us by companies that are seeking to maximize profits at our health – and financial – expense.
Why Traditional Weight Loss Methods Are No Match for “Craveware”
The weight loss industry has thrown everything imaginable at the obesity epidemic: low-fat diets, low-carb diets, point-counting systems, meal replacements, appetite suppressants, and countless “lifestyle programs.” Americans spend over $90 billion annually on weight loss products and services 22. Yet obesity rates continue their relentless climb.
This isn’t a story of lack of willpower or dedication. These approaches rarely consider the psychological and cultural underpinnings that drive our modern eating habits.
The False Promise of Fad Diets
Every few years, a new diet promises to crack the code of sustainable weight loss. Atkins. South Beach. Keto. Paleo. Mediterranean. Each arrives with evangelical fervor and compelling before-and-after photos. Each works brilliantly – for a while 23.
The pattern is remarkably consistent:
Phase 1: Initial rapid weight loss (primarily water)
Phase 2: Slower but continued losses over 3-6 months
Phase 3: Plateau
Phase 4: Gradual regain
Phase 5: Return to baseline weight or higher
The medical literature confirms what millions have experienced firsthand: while any calorie-restricted diet works in the short term, over half the lost weight returns within just two years. 80% of lost weight is regained within five years 24.
But here’s what the glossy diet book covers don’t tell you: each failed attempt leaves people worse off metabolically than if they’d never dieted at all. More on this soon.
Structured Weight Loss Programs: Better, But Not Enough
Commercial weight loss programs like Weight Watchers and Jenny Craig represent a more sophisticated approach. They offer structure, accountability, and some form of behavioral support. Many incorporate evidence-based strategies like regular weigh-ins, food logging, and group support 25.
The results are marginally better than self-directed dieting, but still discouraging: participants enjoy higher initial success rates and slightly better maintenance at one year. However, most participants drop out due to the cost and time commitment and go on to regain significant weight within two years 26. These programs deserve credit for recognizing that sustainable weight loss requires more than just a meal plan. Long-term success hinges on continuous support and behavioral change 27. But they’re still fighting an uphill battle against foods explicitly engineered to override their behavioral strategies.
The Devastating Impact of Weight Cycling
This is where the story takes an unfortunate turn. Each failed weight loss attempt isn’t just a return to square one – it actively damages metabolic health through a process called weight cycling or “yo-yo dieting.”
The cycle is devastating:
Calorie restriction triggers rapid weight loss, and the body loses both fat and lean mass when on restrictive diets 28.
Metabolic rate drops as muscle is lost, slowing or reversing weight loss progress 29.
Intense hunger post-diet can trigger binge eating and weight regain 30.
When weight is regained, it comes back primarily as fat since fat is regained more easily than muscle 31.
Dieters are left worse off metabolically than if they had never tried to lose weight at all 32.
Each weight cycle leaves individuals with a laundry list of ailments:
Body Composition Changes
• Lower muscle mass 33 • Higher body fat percentage 34 • Lower bone mineral density 35 • Increased sarcopenia and frailty 36,37
Studies indicate that the negative impacts of weight cycling (e.g., risk of diabetes, hypertension) may be stronger in women, older adults, and individuals with normal BMI who repeatedly attempt aggressive weight loss 43.
This metabolic damage is compounded by psychological trauma. Each failed attempt reinforces feelings of helplessness and a sense of futility 44. The cruel irony: these negative emotions often trigger comfort eating 45, feeding right into the reward pathways that “craveware” was engineered to exploit.
Truth Is, the Game Was Rigged from the Start
Even the most promising traditional weight loss approaches share a fatal flaw: they require constant vigilance against foods literally designed to break down willpower. Maintaining this vigilance requires ongoing support – regular dietitian meetings, therapy sessions, medical supervision – that few patients or clinicians can sustain indefinitely.
Consider the many resources required for successful long-term weight management:
Regular healthcare provider visits and supervision
Cognitive behavioral therapy or food counseling
Dietitian-led nutrition education and meal planning
Fitness guidance and facilities
Food preparation equipment and time
Social support systems
Now consider that these resources must be maintained indefinitely while navigating a busy life saturated with hyper-convenient, heavily subsidized, hyperpalatable junk foods specifically engineered to trigger overconsumption.
Traditional weight loss methods are simply no match for craveware. These tools place the entire burden of behavior change on individuals while ignoring the sophisticated Big Tobacco addiction playbook that created the problem in the first place.
If we were to have any hope for success in the war on obesity, we needed a new class of tools powerful enough to counter industrially engineered food cravings.
An Investigation into the Hidden Realities of the War on Obesity and the Food Industrial Complex.
This is a preview of our forthcoming three-part series on The Ozempic Era. This series explores how the Food Industrial Complex engineered an addiction crisis, how Ozempic emerged as its apparent antidote, and why millions of desperate patients betting their health on GLP-1 drugs may be making a deal with the devil.
Introducing The Ozempic Era
Obesity has eaten the world. Over 40% of American adults now live with obesity 1 – a more than threefold increase from the 13% recorded in the early 1960s 2. Today, nearly three-quarters of Americans are considered overweight or obese. The numbers are staggering, almost incomprehensible in their scale: in just two generations, we’ve witnessed the most dramatic transformation of human bodies in recorded history.
But this isn’t just an American story anymore. What began as a crisis of affluence in Western nations has morphed into a global pandemic that defies old assumptions about wealth, culture, and diet. China and Saudi Arabia 3, riding waves of newfound prosperity, have seen obesity rates skyrocket as they’ve adopted the trappings of Western consumer culture. More shocking still, regions of the world that were battling undernourishment just decades ago – from Latin America to sub-Saharan Africa to Southeast Asia – now find themselves inundated with an excess of cheap, empty calories 4.
This unprecedented reshaping of human bodies isn’t a crisis of willpower – it’s a hijacking. Over the past 50 years, multinational food conglomerates have used Big Tobacco’s addiction playbook to dismantle traditional foods and replace them with “craveware” – highly addictive food products specifically designed to hack our brain’s reward circuitry and drive compulsive consumption 5.
The result? Over the past 50 years, we’ve witnessed a seismic shift in global diets, marked by an ever-increasing reliance on processed foods, meals eaten away from home, and the ubiquitous presence of edible oils and sugar-sweetened beverages 6. This transformation accelerated with globalization, as transnational food conglomerates exported their highly addictive, ultra-processed products to every corner of the globe.
For decades, the weight loss industry has thrown everything but the kitchen sink at this problem. Fad diets, meal replacement shakes, point-counting systems, appetite suppressants, major surgeries – each promising to be the silver bullet that would finally reverse the tide of global obesity 7. Each, in turn, proved inadequate against the overwhelming force of the Food Industrial Complex’s craveware.
Enter Ozempic.
Unlike the milquetoast weight loss solutions of yesteryear, GLP-1 agonists like Ozempic represent something genuinely revolutionary: a pharmaceutical intervention that delivers significant, sustained weight loss for a substantial number of users. Clinical trials show participants losing up to 15% of their body weight over 68 weeks with semaglutide (Ozempic/Wegovy) 8, while its newer cousin tirzepatide (Mounjaro/Zepbound) pushes that number to 20% or more 9. These aren’t just numbers on a scale – they represent meaningful improvements in health outcomes, including enhanced longevity and improved quality of life.
For the first time, we have a tool that seems capable of undoing the damage inflicted by five decades of industrial food engineering. The excitement is palpable among both medical professionals and patients, leading to an explosion in prescriptions for weight loss 10. An emerging body of evidence even indicates these drugs may help treat a broad category of other addictions, from alcohol to drugs to gambling 11, leading to breathless headlines about Ozempic as a panacea for human cravings.
But there’s a dark side to this “miracle drug” that the headlines often miss. Beyond the well-documented side effects of Ozempic – from gastrointestinal issues 12 to catastrophic loss of muscle mass 13 – lies an even more troubling reality: these drugs are failing to uphold their end of the weight loss bargain in the long run.
The terms of this Faustian bargain are becoming increasingly clear. The drugs work brilliantly, but only for as long as patients keep taking them. Yet data shows the majority of patients cease using these drugs within a year 14, due to a combination of high costs and poor insurance coverage 15, onerous side effects 16, and persistent supply issues. This combination of factors often leaves people worse off physically, mentally, and financially than before they began treatment. But most devastating of all, the weight loss progress they achieved – the very purpose of this bargain – typically vanishes within months of stopping the medication 17. And their bodies are left worse for the wear.
Part I of “The Ozempic Era” series reveals how the Food Industrial Complex engineered hyper-addictive “craveware” foods that have hacked the brains of billions and fueled the obesity crisis.
Part II of the series explores the emergence of “miracle” weight loss medications as an apparent panacea for not just obesity but all addictive behaviors – if you’re willing to pay the price.
Finally, Part III of the series digs deeper into the Ozempic story and uncovers an unsettling reality: the millions of desperate patients who turning to GLP-1 drugs may be making a deal with the devil.

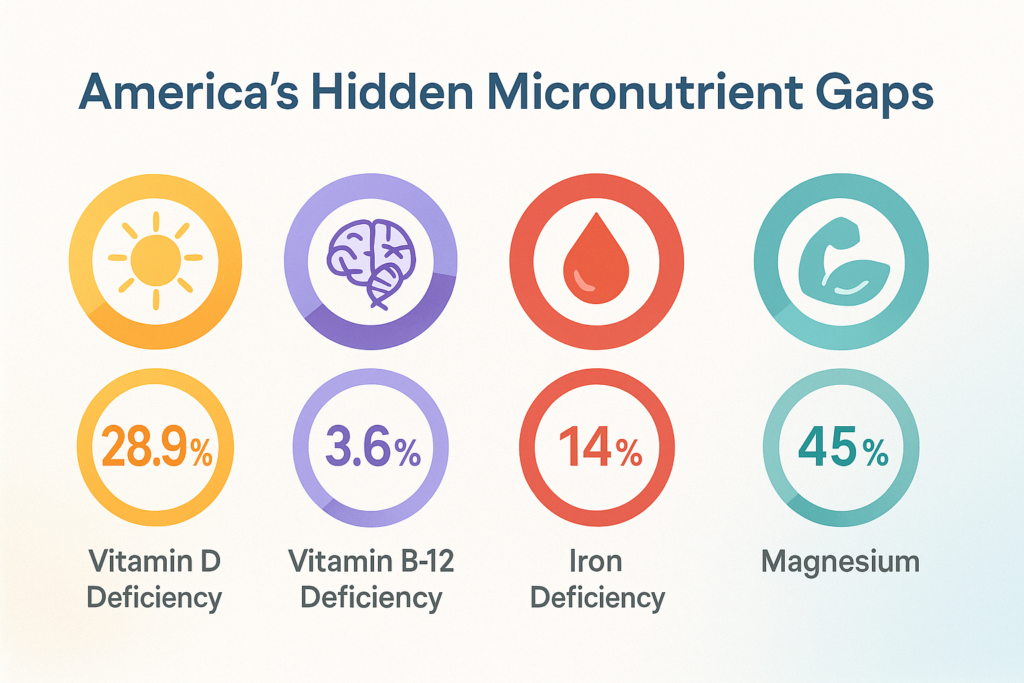







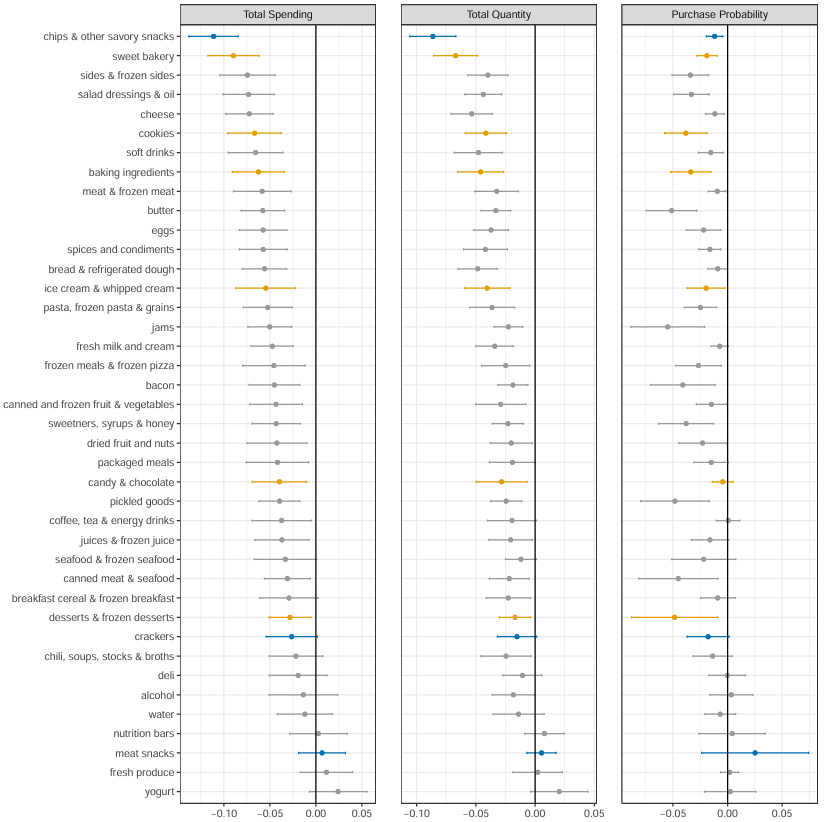
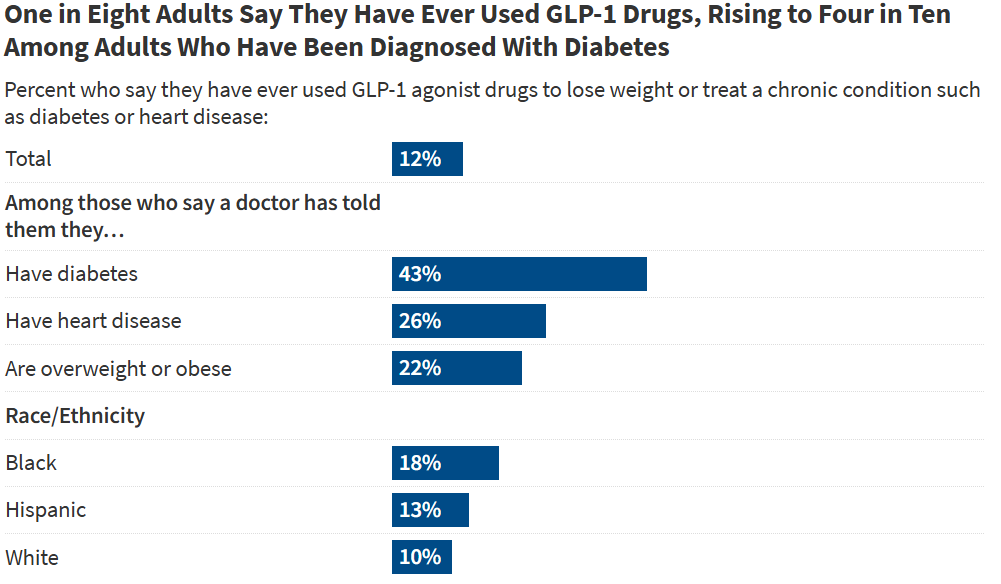


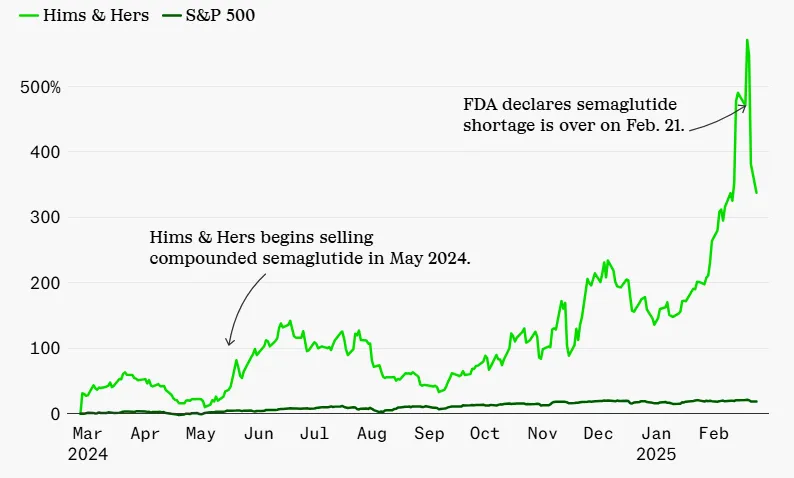
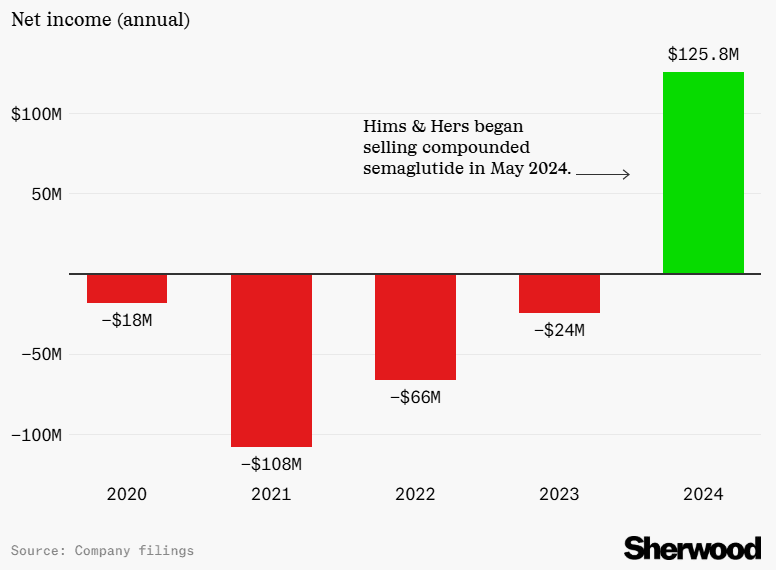
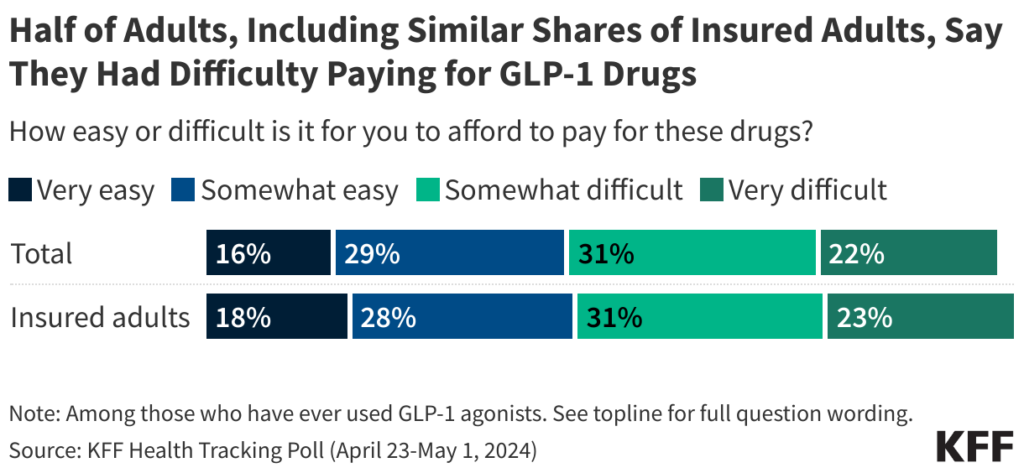
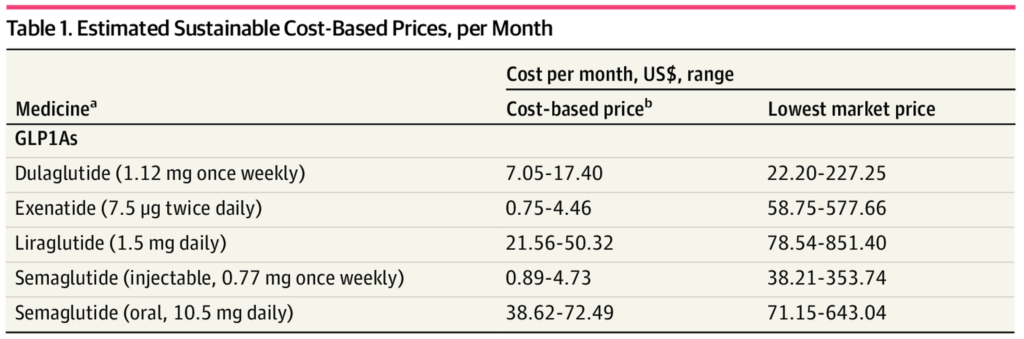
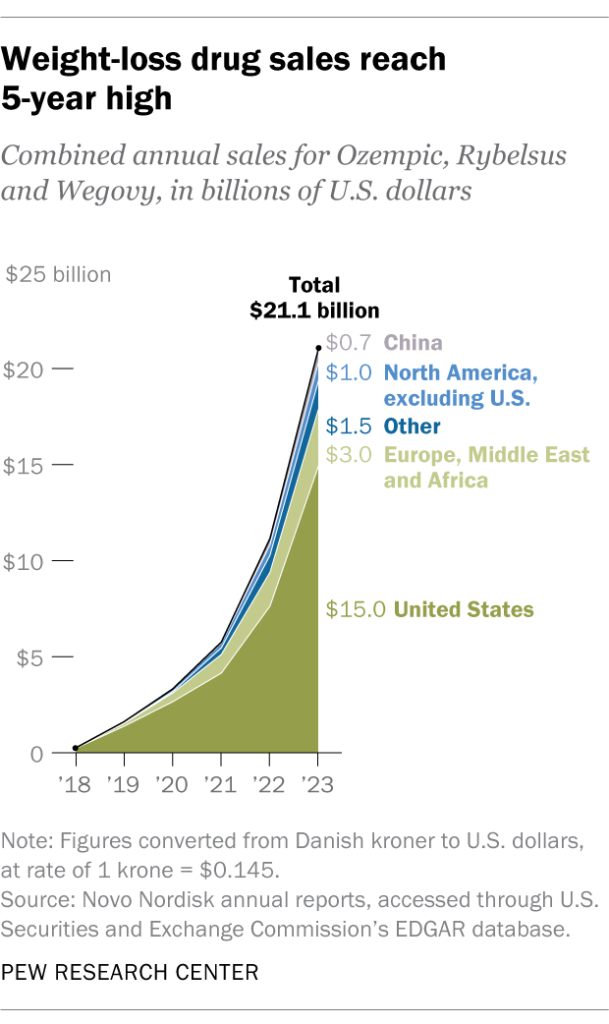
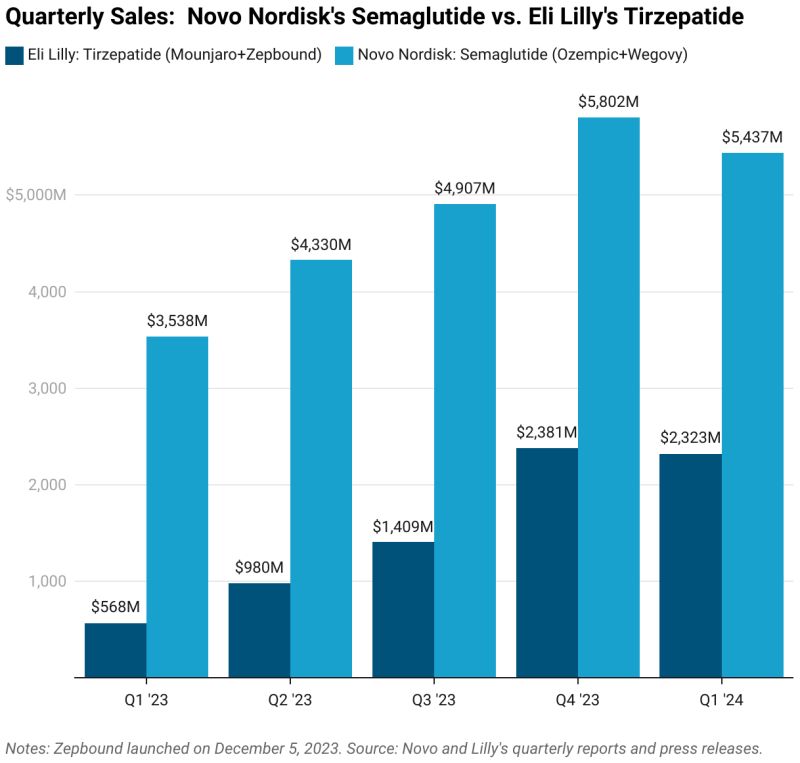
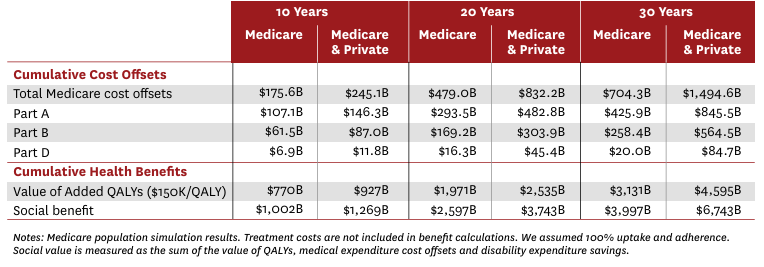
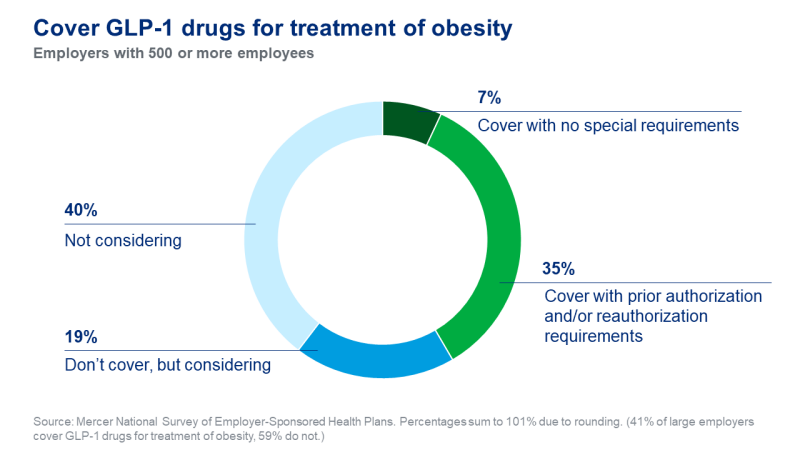
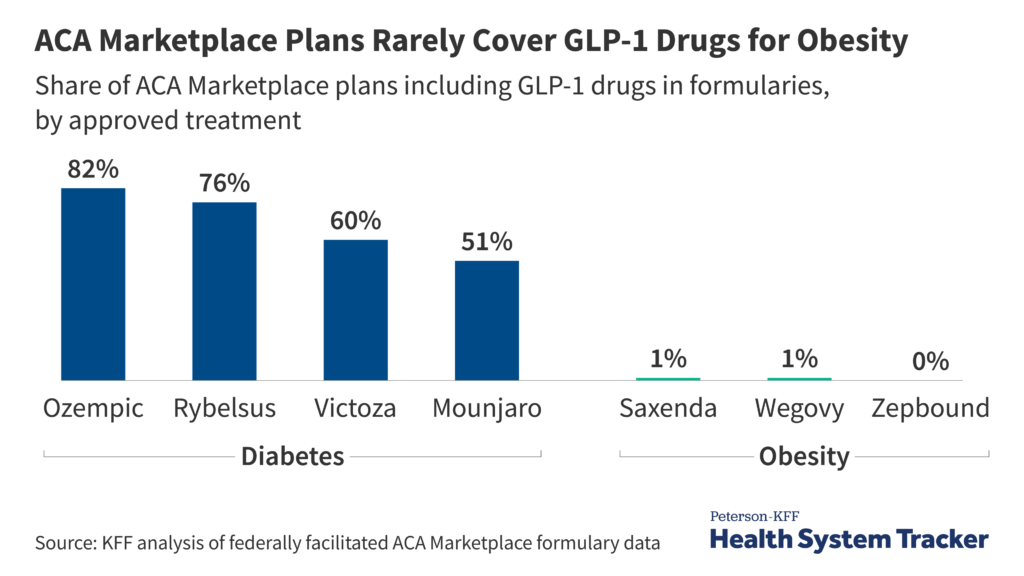
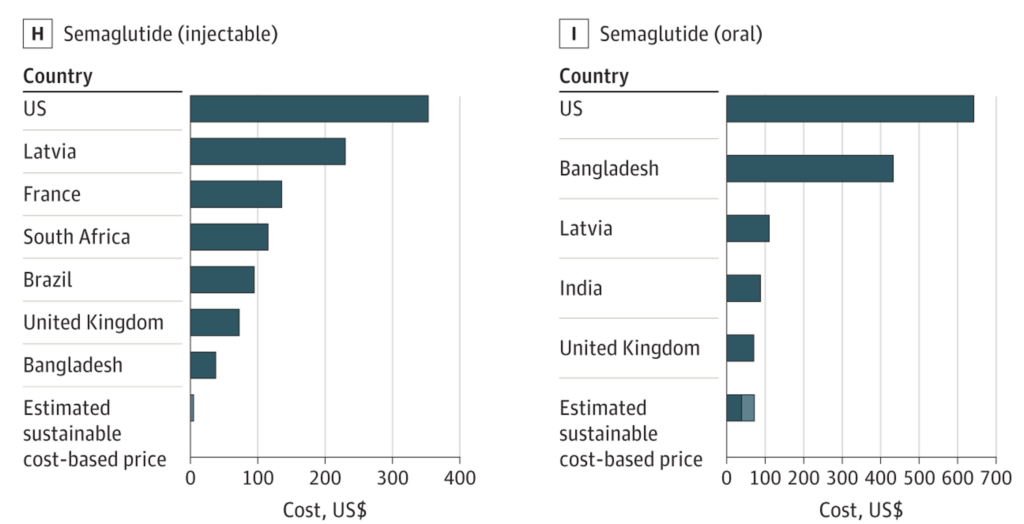





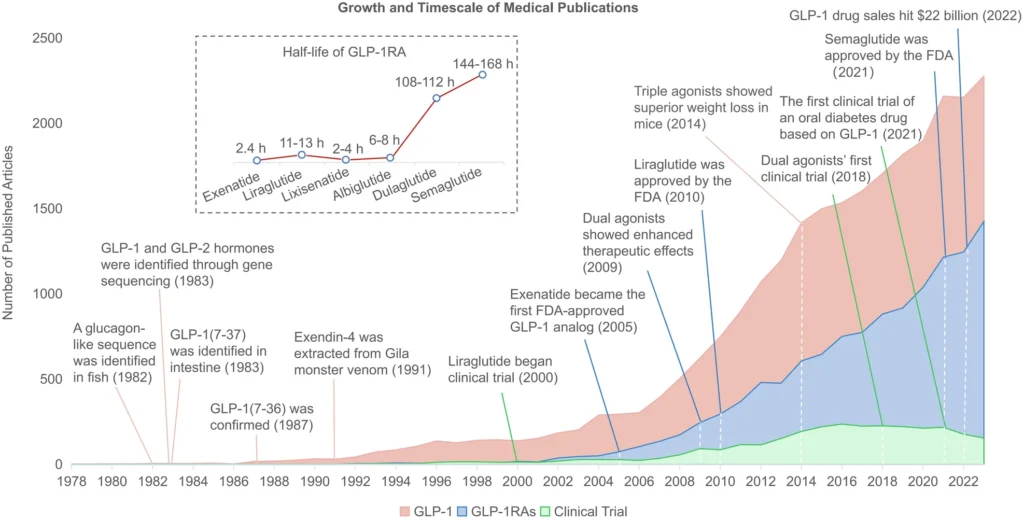
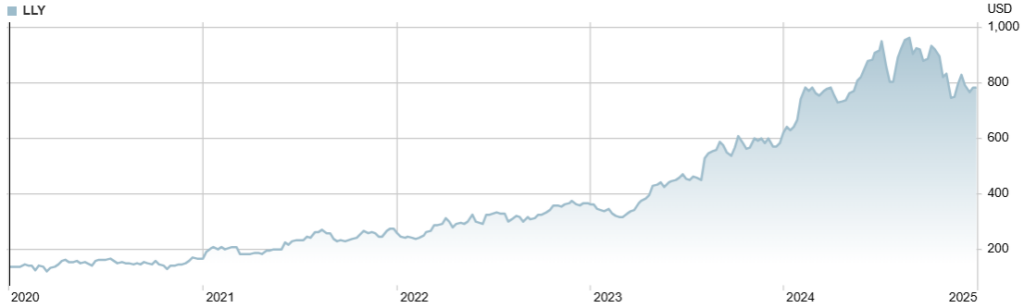

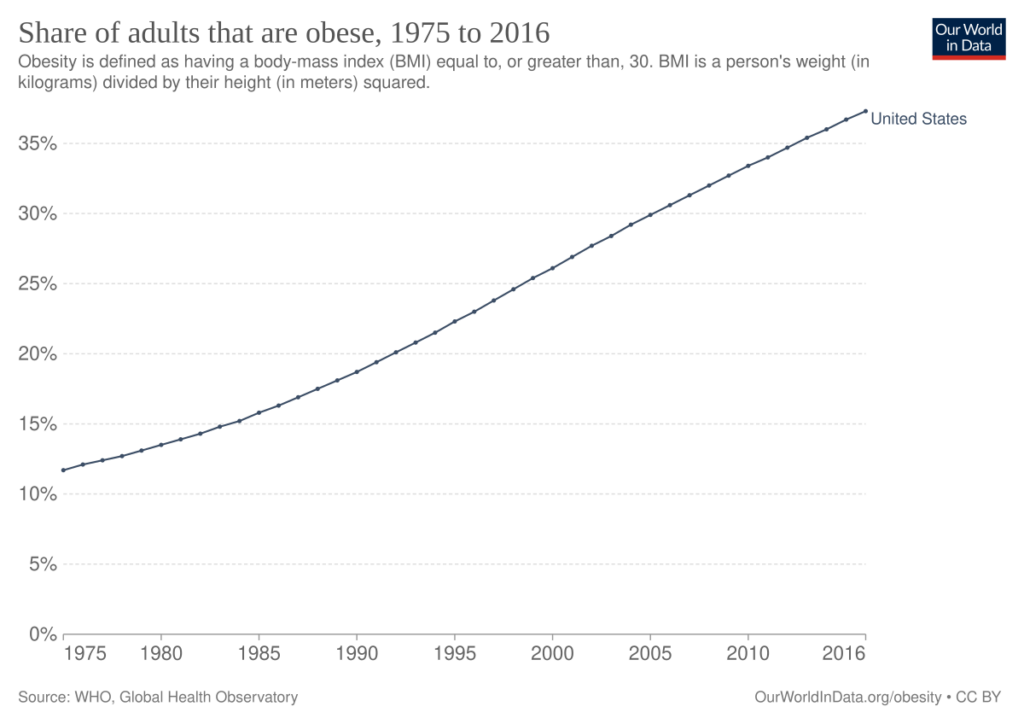

{kind=link}